

Lack of a Tricuspid Regurgitation Doppler Signal and Pulmonary Hypertension by Invasive Measurement
- PMID: 29960993
- PMCID: PMC6064901
- DOI: 10.1161/JAHA.118.009362
Lack of a Tricuspid Regurgitation Doppler Signal and Pulmonary Hypertension by Invasive Measurement
Abstract
Background: Transthoracic echocardiography (TTE) is used to estimate pulmonary artery systolic pressure, but an adequate tricuspid regurgitation velocity (TRV) needed to calculate pulmonary artery systolic pressure is not always present. It is unknown whether the absence of a measurable TRV signifies normal pulmonary artery pressure.
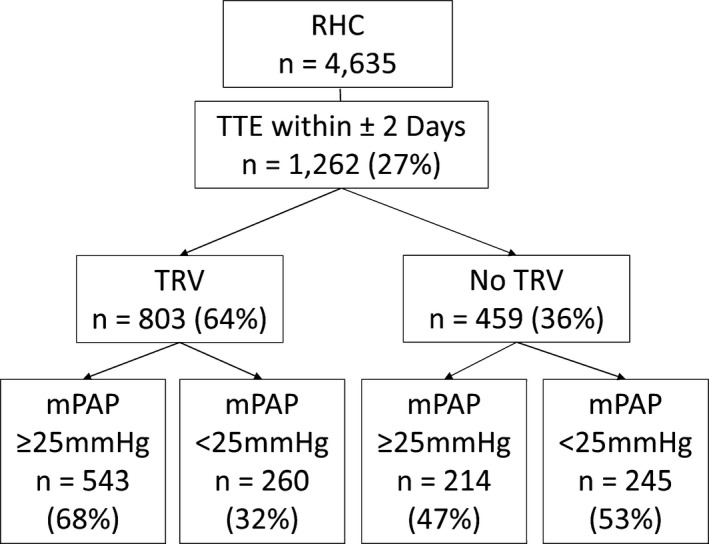
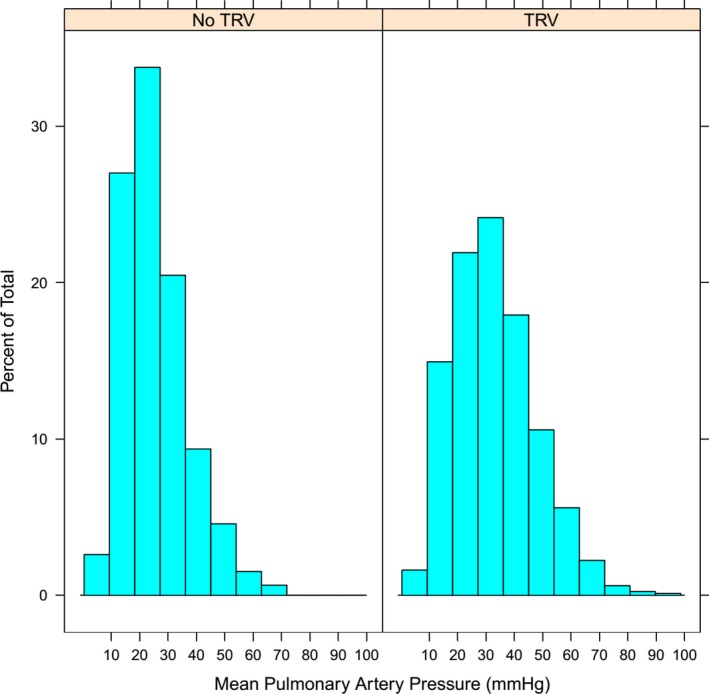
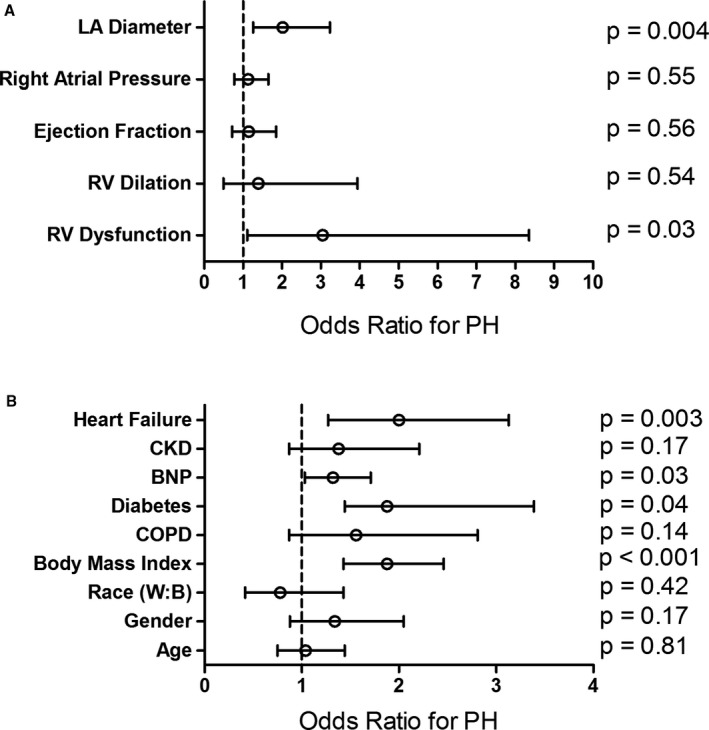
Methods and results: We extracted hemodynamic, TTE, and clinical data from Vanderbilt's deidentified electronic medical record in all patients referred for right heart catheterization between 1998 and 2014. Pulmonary hypertension (PH) was defined as mean pulmonary artery pressure ≥25 mm Hg. We examined the prevalence and clinical correlates of PH in patients without a reported TRV. We identified 1262 patients with a TTE within 2 days of right heart catheterization. In total, 803/1262 (64%) had a reported TRV, whereas 459 (36%) had no reported TRV. Invasively confirmed PH was present in 47% of patients without a reported TRV versus 68% in those with a reported TRV (P<0.001). Absence of a TRV yielded a negative predictive value for excluding PH of 53%. Right ventricular dysfunction, left atrial dimension, elevated body mass index, higher brain natriuretic peptide, diabetes mellitus, and heart failure were independently associated with PH among patients without a reported TRV.
Conclusions: PH is present in almost half of patients without a measurable TRV who are referred for both TTE and right heart catheterization. Clinical and echocardiographic features of left heart disease are associated with invasively confirmed PH in subjects without a reported TRV. Clinicians should use caution when making assumptions about PH status in the absence of a measurable TRV on TTE.
Keywords: echocardiography; hemodynamics; imaging; pulmonary hypertension; right heart catheterization.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) , Galiè N, Humbert M, Vachiery J‐L, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur Heart J. 2016; 37:67–119. - PubMed
-
- Simonneau G, Galiè N, Rubin LJ, Langleben D, Seeger W, Domenighetti G, Gibbs S, Lebrec D, Speich R, Beghetti M, Rich S, Fishman A. Clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2004;43:5S–12S. - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, Mathier MA, McGoon MD, Park MH, Rosenson RS, Rubin LJ, Tapson VF, Varga J. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc; and the Pulmonary Hypertension Association. Circulation. 2009;119:2250–2294. - PubMed
-
- Zoghbi WA, Enriquez‐Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, Rakowski H, Stewart WJ, Waggoner A, Weissman NJ. Recommendations for evaluation of the severity of native valvular regurgitation with two‐dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777–802. - PubMed
-
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713; quiz 786–788. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
