

Long-Term Mortality of Older Patients With Acute Myocardial Infarction Treated in US Clinical Practice
- PMID: 29960995
- PMCID: PMC6064921
- DOI: 10.1161/JAHA.117.007230
Long-Term Mortality of Older Patients With Acute Myocardial Infarction Treated in US Clinical Practice
Abstract
Background: There is limited information about the long-term survival of older patients after myocardial infarction (MI).
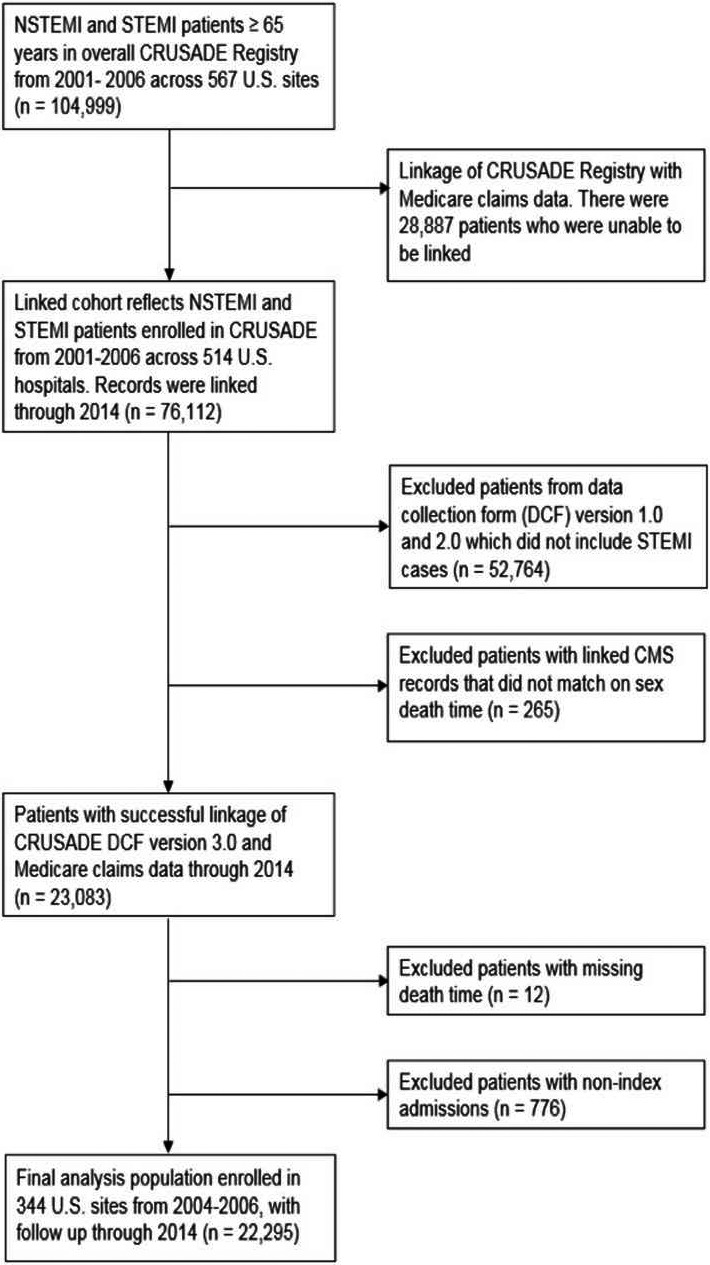
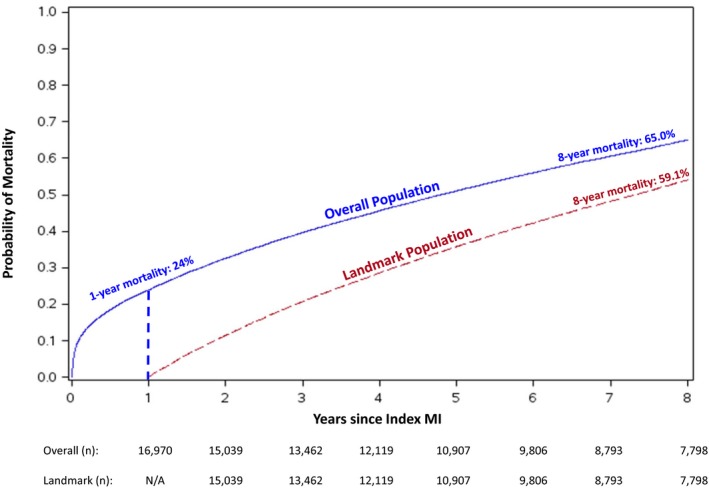
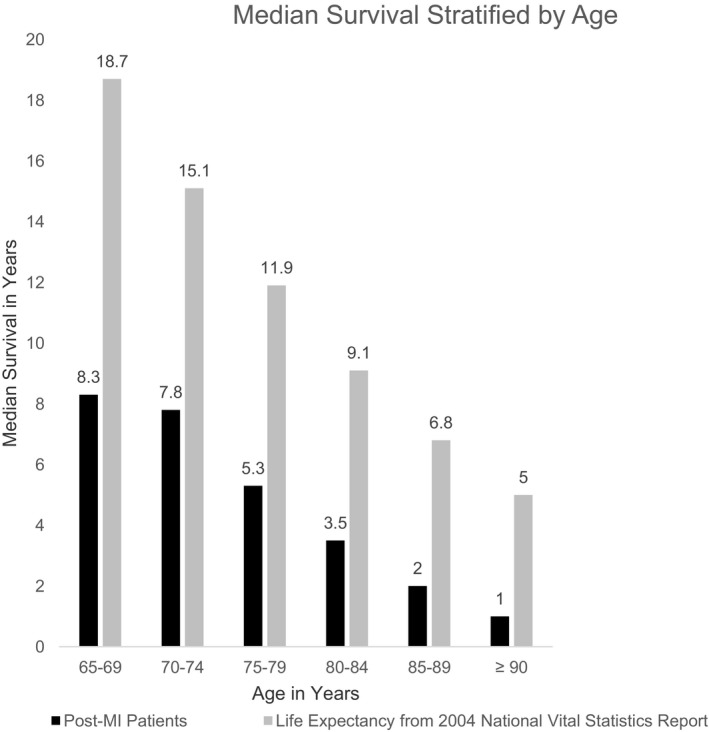
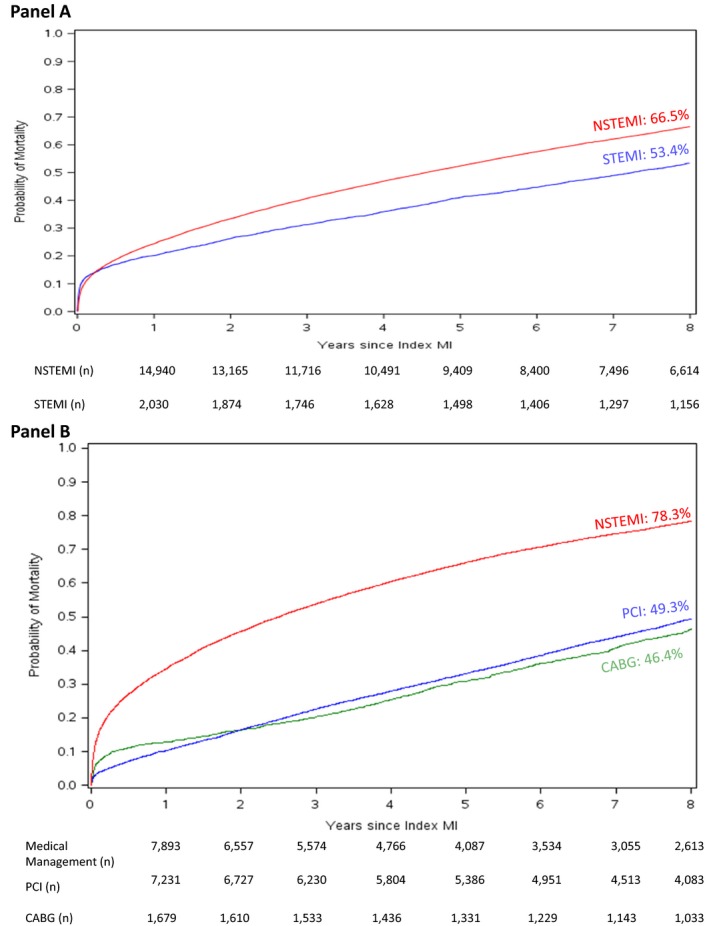
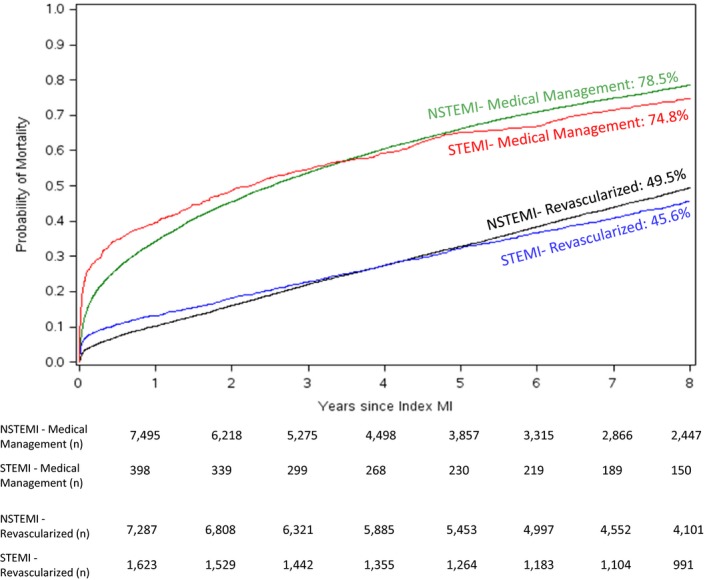
Methods and results: CRUSADE (Can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the ACC/AHA guidelines) was a registry of MI patients treated at 568 US hospitals from 2001 to 2006. We linked MI patients aged ≥65 years in CRUSADE to their Medicare data to ascertain long-term mortality (defined as 8 years post index event). Long-term unadjusted Kaplan-Meier mortality curves were examined among patients stratified by revascularization status. A landmark analysis conditioned on surviving the first year post-MI was conducted. We used multivariable Cox regression to compare mortality risks between ST-segment-elevation myocardial infarction and non-ST-segment-elevation myocardial infarction patients. Among 22 295 MI patients ≥ age 65 years (median age 77 years), we observed high rates of evidence-based medication use at discharge: aspirin 95%, β-blockers 94%, and statins 81%. Despite this, mortality rates were high: 24% at 1 year, 51% at 5 years, and 65% at 8 years. Eight-year mortality remained high among patients who underwent percutaneous coronary intervention (49%), coronary artery bypass graft (46%), and among patients who survived the first year post-MI (59%). Median survival was 4.8 years (25th, 75th percentiles 1.1, 8.5); among patients aged 65-74 years it was 8.2 years (3.3, 8.9) while for patients aged ≥75 years it was 3.1 years (0.6, 7.6). Eight-year mortality was lower among ST-segment-elevation myocardial infarction than non-ST-segment-elevation myocardial infarction patients (53% versus 67%); this difference was not significant after adjustment (hazard ratio 0.94, 95% confidence interval, 0.88-1.00).
Conclusions: Long-term mortality remains high among patients with MI in routine clinical practice, even among revascularized patients and those who survived the first year.
Keywords: elderly; mortality; myocardial infarction; revascularization; survival.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Alexander KP, Newby LK, Cannon CP, Armstrong PW, Gibler WB, Rich MW, Van de Werf F, White HD, Weaver WD, Naylor MD, Gore JM, Krumholz HM, Ohman EM; American Heart Association Council on Clinical Cardiology; Society of Geriatric Cardiology . Acute coronary care in the elderly, part I: non‐ST‐segment‐elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2549–2569. - PubMed
-
- Tegn N, Abdelnoor M, Aaberge L, Endresen K, Smith P, Aakhus S, Gjertsen E, Dahl‐Hofseth O, Ranhoff AH, Gullestad L, Bendz B; After Eighty study Investigators . Invasive versus conservative strategy in patients aged 80 years or older with non‐ST‐elevation myocardial infarction or unstable angina pectoris (After Eighty study): an open‐label randomised controlled trial. Lancet. 2016;387:1057–1065. - PubMed
-
- Velders MA, James SK, Libungan B, Sarno G, Frobert O, Carlsson J, Schalij MJ, Albertsson P, Lagerqvist B. Prognosis of elderly patients with ST‐elevation myocardial infarction treated with primary percutaneous coronary intervention in 2001 to 2011: a report from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR) registry. Am Heart J. 2014;167:666–673. - PubMed
-
- Viana‐Tejedor A, Loughlin G, Fernandez‐Aviles F, Bueno H. Temporal trends in the use of reperfusion therapy and outcomes in elderly patients with first ST elevation myocardial infarction. Eur Heart J‐Acute Ca. 2015;4:461–467. - PubMed
-
- Hoekstra JW, Pollack CV Jr, Roe MT, Peterson ED, Brindis R, Harrington RA, Christenson RH, Smith SC, Ohman EM, Gibler WB. Improving the care of patients with non‐ST‐elevation acute coronary syndromes in the emergency department: the CRUSADE initiative. Acad Emerg Med. 2002;9:1146–1155. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
