

Acute kidney injury in the UK: a replication cohort study of the variation across three regional populations
- PMID: 29961002
- PMCID: PMC6042563
- DOI: 10.1136/bmjopen-2017-019435
Acute kidney injury in the UK: a replication cohort study of the variation across three regional populations
Abstract
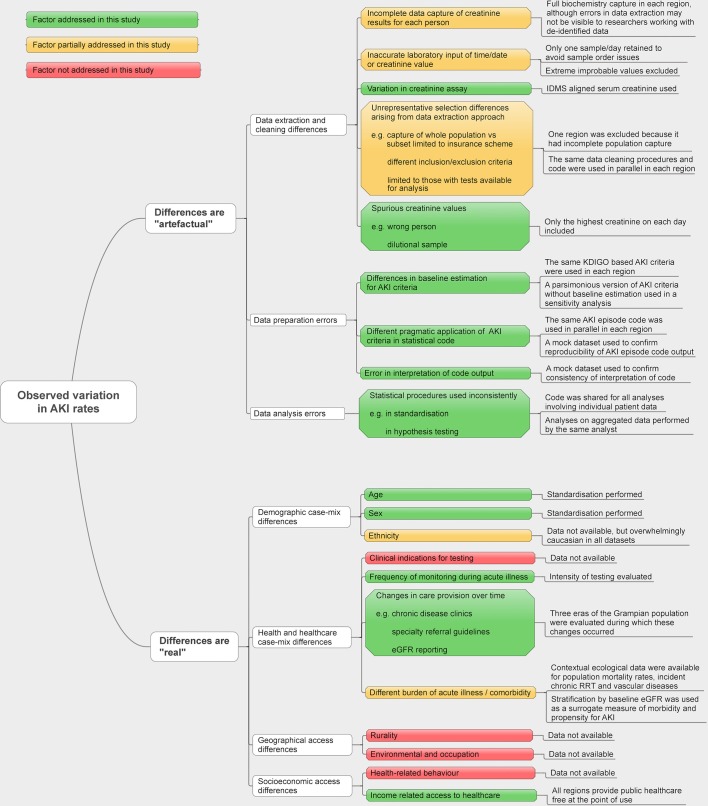
Objectives: A rapid growth in the reported rates of acute kidney injury (AKI) has led to calls for greater attention and greater resources for improving care. However, the reported incidence of AKI also varies more than tenfold between previous studies. Some of this variation is likely to stem from methodological heterogeneity. This study explores the extent of cross-population variation in AKI incidence after minimising heterogeneity.
Design: Population-based cohort study analysing data from electronic health records from three regions in the UK through shared analysis code and harmonised methodology.
Setting: Three populations from Scotland, Wales and England covering three time periods: Grampian 2003, 2007 and 2012; Swansea 2007; and Salford 2012.
Participants: All residents in each region, aged 15 years or older.
Main outcome measures: Population incidence of AKI and AKI phenotype (severity, recovery, recurrence). Determined using shared biochemistry-based AKI episode code and standardised by age and sex.
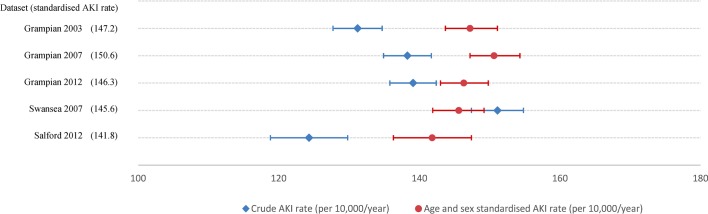
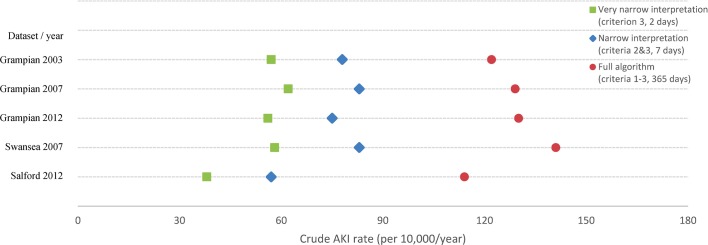
Results: Respectively, crude AKI rates (per 10 000/year) were 131, 138, 139, 151 and 124 (p=0.095), and after standardisation for age and sex: 147, 151, 146, 146 and 142 (p=0.257) for Grampian 2003, 2007 and 2012; Swansea 2007; and Salford 2012. The pattern of variation in crude rates was robust to any modifications of the AKI definition. Across all populations and time periods, AKI rates increased substantially with age from ~20 to ~550 per 10 000/year among those aged <40 and ≥70 years.
Conclusion: When harmonised methods are used and age and sex differences are accounted for, a similar high burden of AKI is consistently observed across different populations and time periods (~150 per 10 000/year). There are particularly high rates of AKI among older people. Policy-makers should be careful not draw simplistic assumptions about variation in AKI rates based on comparisons that are not rigorous in methodological terms.
Keywords: acute renal failure; epidemiology; nephrology; public health.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: DN reports grants from Informatica for analyses of the National CKD Audit, which was tendered by HQIP (funding from NHS Wales and NHS England), outside the submitted work. SS is supported by a research training fellowship from the Wellcome Trust to study the outcomes of acute kidney injury (WT102729/Z/13/Z). No other support from any organisation for the submitted work; no other financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
- MR/ K006584/1/MRC_/Medical Research Council/United Kingdom
- BHF_/British Heart Foundation/United Kingdom
- MC_PC_13042/MRC_/Medical Research Council/United Kingdom
- MC_PC_13043/MRC_/Medical Research Council/United Kingdom
- WT102729/Z/13/Z/WT_/Wellcome Trust/United Kingdom
- MC_UU_12011/3/MRC_/Medical Research Council/United Kingdom
- CRUK_/Cancer Research UK/United Kingdom
- MR/K006665/1/MRC_/Medical Research Council/United Kingdom
- ARC_/Arthritis Research UK/United Kingdom
- MR/K006525/1/MRC_/Medical Research Council/United Kingdom
- MC_UP_A620_1016/MRC_/Medical Research Council/United Kingdom
- MR/K007017/1/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- CSO_/Chief Scientist Office/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases