

Prognostic significance of frequent CLDN18-ARHGAP26/6 fusion in gastric signet-ring cell cancer
- PMID: 29961079
- PMCID: PMC6026495
- DOI: 10.1038/s41467-018-04907-0
Prognostic significance of frequent CLDN18-ARHGAP26/6 fusion in gastric signet-ring cell cancer
Abstract
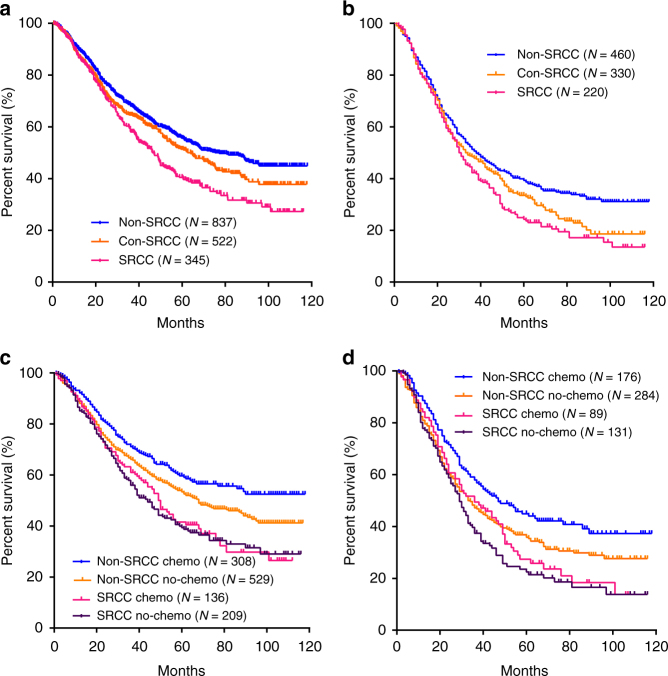
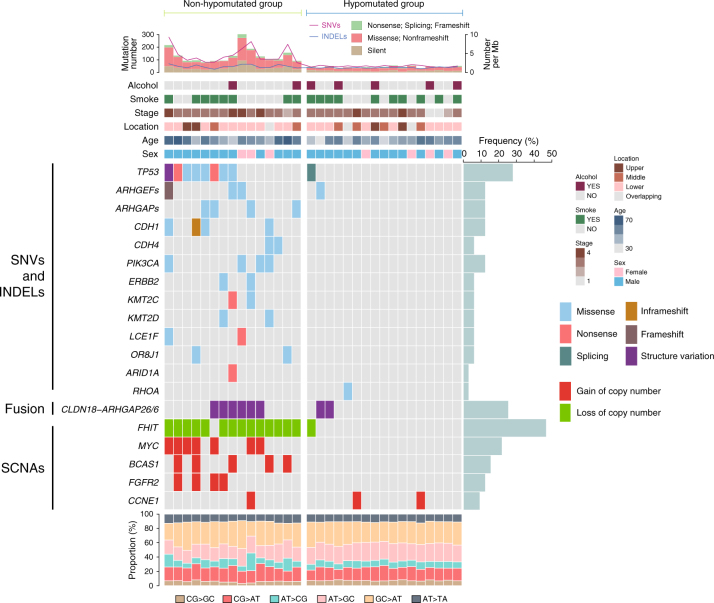
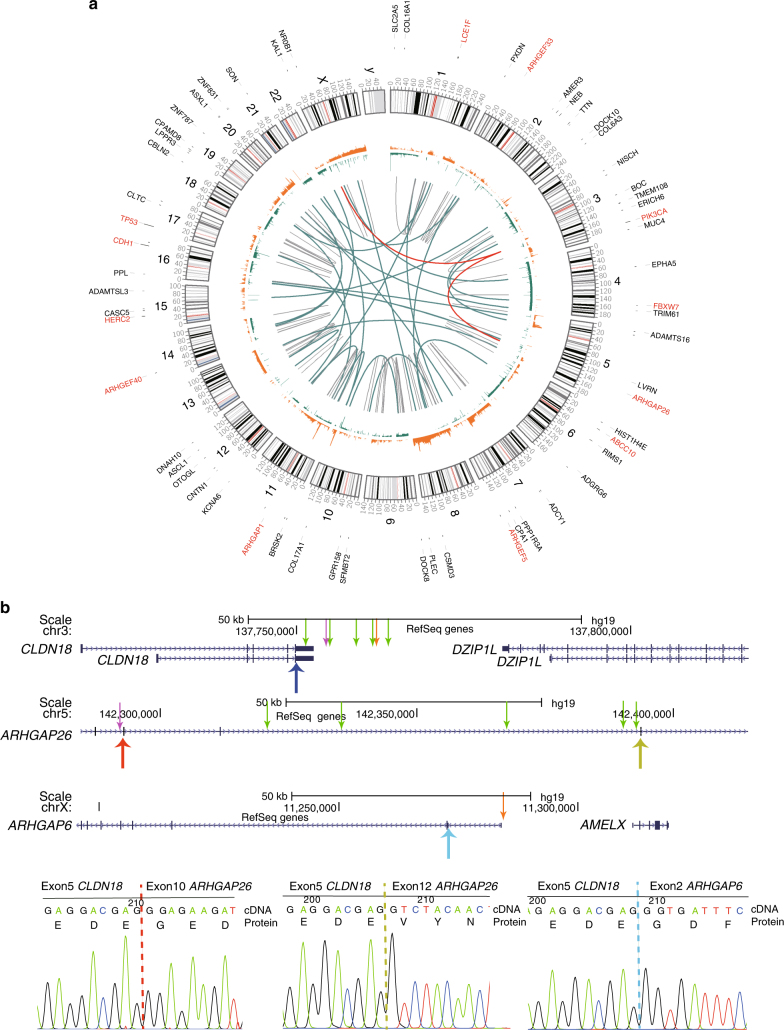
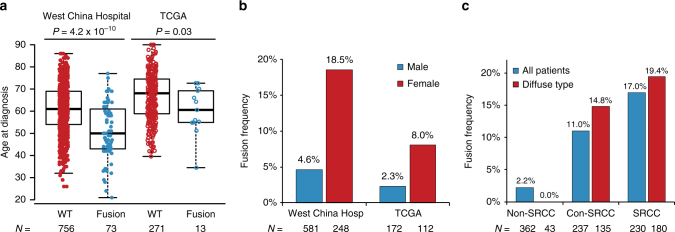
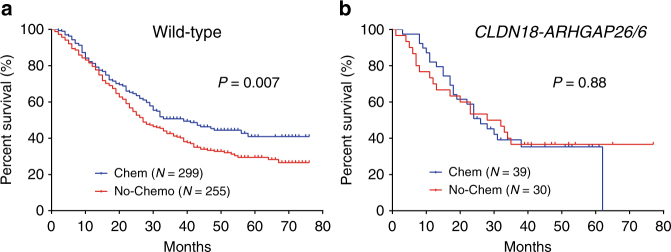
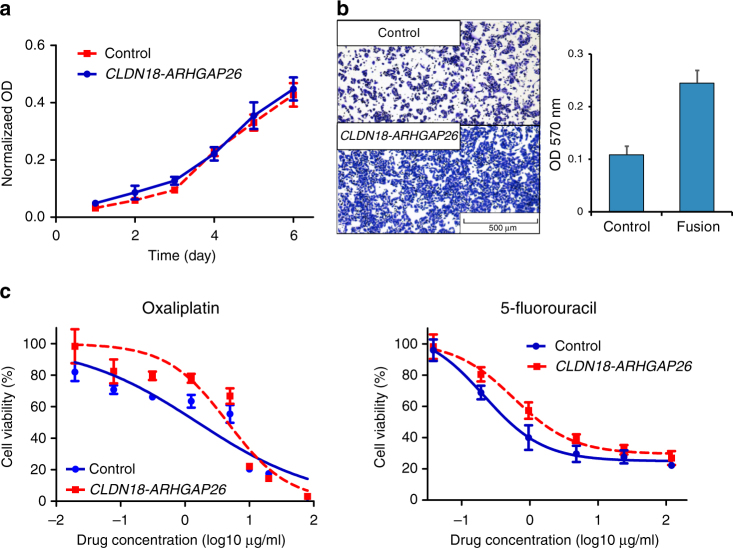
Signet-ring cell carcinoma (SRCC) has specific epidemiology and oncogenesis in gastric cancer, however, with no systematical investigation for prognostic genomic features. Here we report a systematic investigation conducted in 1868 Chinese gastric cancer patients indicating that signet-ring cells content was related to multiple clinical characteristics and treatment outcomes. We thus perform whole-genome sequencing on 32 pairs of SRC samples, and identify frequent CLDN18-ARHGAP26/6 fusion (25%). With 797 additional patients for validation, prevalence of CLDN18-ARHGAP26/6 fusion is noticed to be associated with signet-ring cell content, age at diagnosis, female/male ratio, and TNM stage. Importantly, patients with CLDN18-ARHGAP26/6 fusion have worse survival outcomes, and get no benefit from oxaliplatin/fluoropyrimidines-based chemotherapy, which is consistent with the fact of chemo-drug resistance acquired in CLDN18-ARHGAP26 introduced cell lines. Overall, this study provides insights into the clinical and genomic features of SRCC, and highlights the importance of frequent CLDN18-ARHGAP26/6 fusions in chemotherapy response for SRCC.
Conflict of interest statement
Hongye Sun, Hua Cheng, and Bin Zheng are employees of WuxiNextCODE. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
