

Radiotherapy dose-volume parameters predict videofluoroscopy-detected dysphagia per DIGEST after IMRT for oropharyngeal cancer: Results of a prospective registry
- PMID: 29961581
- PMCID: PMC6595477
- DOI: 10.1016/j.radonc.2018.06.013
Radiotherapy dose-volume parameters predict videofluoroscopy-detected dysphagia per DIGEST after IMRT for oropharyngeal cancer: Results of a prospective registry
Abstract
Purpose: Our primary aim was to prospectively validate retrospective dose-response models of chronic radiation-associated dysphagia (RAD) after intensity modulated radiotherapy (IMRT) for oropharyngeal cancer (OPC). The secondary aim was to validate a grade ≥2 cut-point of the published videofluoroscopic dysphagia severity (Dynamic Imaging Grade for Swallowing Toxicity, DIGEST) as radiation dose-dependent.
Material and methods: Ninety-seven patients enrolled on an IRB-approved prospective registry protocol with stage I-IV OPC underwent pre- and 3-6 month post-RT videofluoroscopy. Dose-volume histograms (DVH) for swallowing regions of interest (ROI) were calculated. Dysphagia severity was graded per DIGEST criteria (dichotomized with grade ≥2 as moderate/severe RAD). Recursive partitioning analysis (RPA) and Bayesian Information Criteria (BIC) were used to identify dose-volume effects associated with moderate/severe RAD.
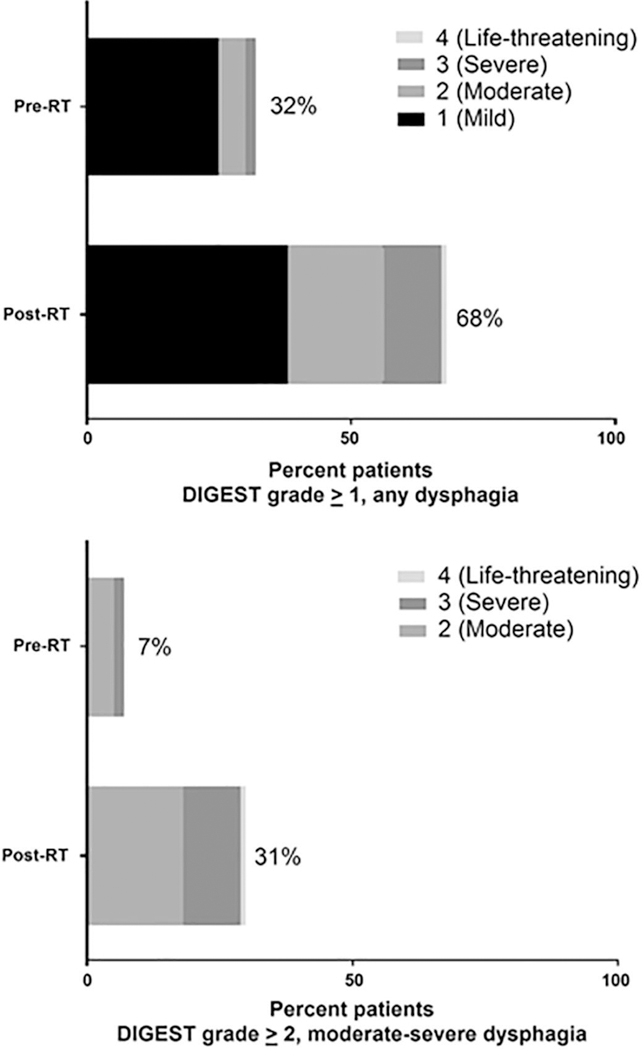
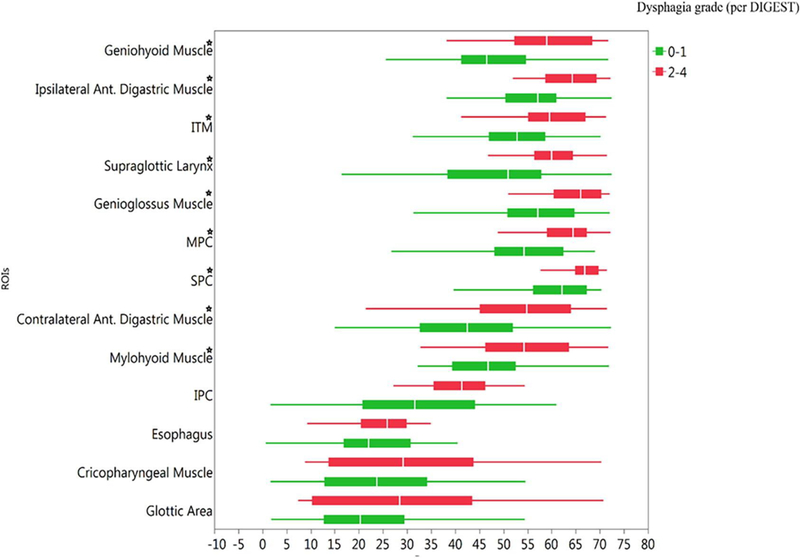
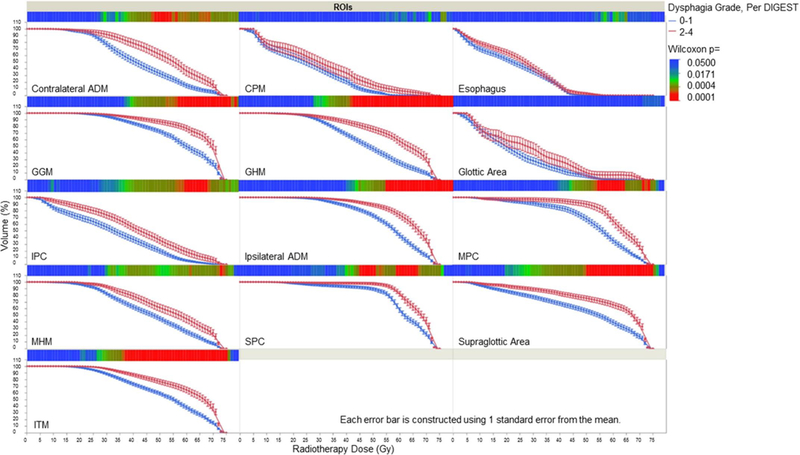
Results: 31% developed moderate/severe RAD (i.e. DIGEST grade ≥2) at 3-6 months after RT. RPA found DVH-derived dosimetric parameters of geniohyoid/mylohyoid (GHM), superior pharyngeal constrictor (SPC), and supraglottic region were associated with DIGEST grade ≥2 RAD. V61 ≥ 18.57% of GHM demonstrated optimal model performance for prediction of DIGEST grade ≥2.
Conclusion: The findings from this prospective longitudinal registry validate prior observations that dose to submental musculature predicts for increased burden of dysphagia after oropharyngeal IMRT. Findings also support dichotomization of DIGEST grade ≥2 as a dose-dependent split for use as an endpoint in trials or predictive dose-response analysis of videofluoroscopy results.
Keywords: DIGEST; Dose–volume; Dysphagia; Intensity-modulated radiation therapy; Oropharyngeal cancer; Radiotherapy.
Copyright © 2018 Elsevier B.V. All rights reserved.
Figures
References
-
- Garden AS, Dong L, Morrison WH, Stugis EM, Glisson BS, Frank SJ, et al. Patterns of disease recurrence following treatment of oropharyngeal cancer with intensity modulated radiation therapy.Int J Radiat Oncol Biol Phys 2013;85:941–7. - PubMed
-
- Daly ME, Le Q-T, Maxim PG, Loo BW, Kaplan MJ, Fischbein NJ, et al. Intensity-modulated Radiotherapy in the treatment of oropharyngeal cancer: clinical outcomes and patterns of failure. Int J Radiat Oncol Biol Phys 2010;76:1339–46. - PubMed
-
- Parsons JT, Mendenhall WM, Stringer SP, Amdur RJ, Hinerman RW, Villaret DB, et al. Squamous cell carcinoma of the oropharynx. Cancer 2002;94:2967–80. - PubMed
-
- Bhayani MK, Hutcheson KA, Barringer DA, Lisec A, Alvarez CP, Roberts DB, et al. Gastrostomy tube placement in patients with oropharyngeal carcinoma treated with radiotherapy or chemoradiotherapy: factors affecting placement and dependence. Head Neck 2013;35:1634–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
