

Comparison between uncut Roux-en-Y and Roux-en-Y reconstruction after distal gastrectomy for gastric cancer: A meta-analysis
- PMID: 29962819
- PMCID: PMC6021772
- DOI: 10.3748/wjg.v24.i24.2628
Comparison between uncut Roux-en-Y and Roux-en-Y reconstruction after distal gastrectomy for gastric cancer: A meta-analysis
Abstract
Aim: To compare uncut Roux-en-Y (U-RY) gastrojejunostomy with Roux-en-Y (RY) gastrojejunostomy after distal gastrectomy (DG) for gastric cancer.
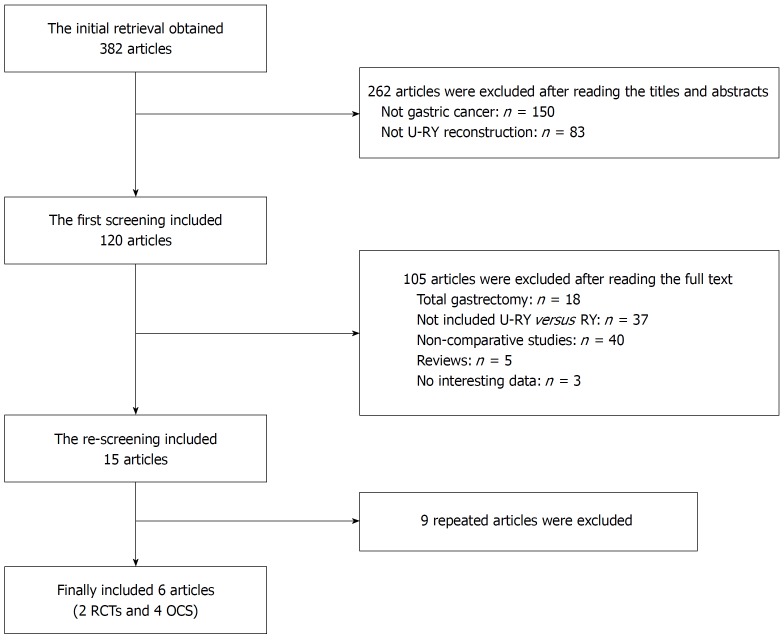
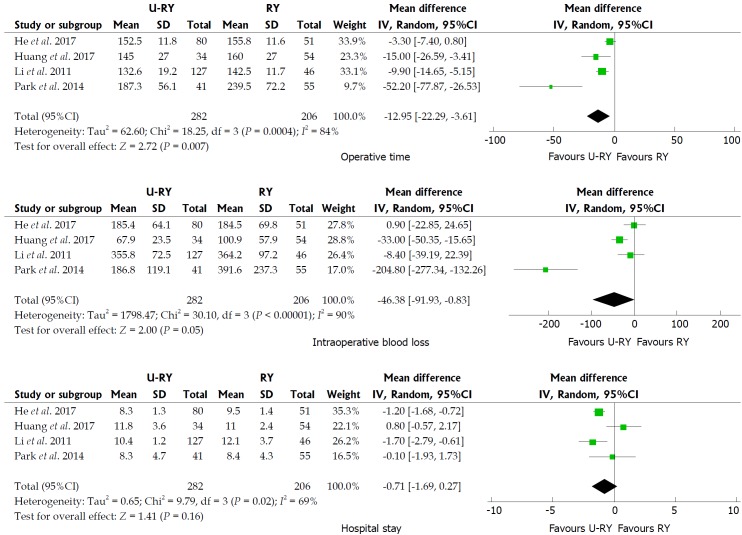
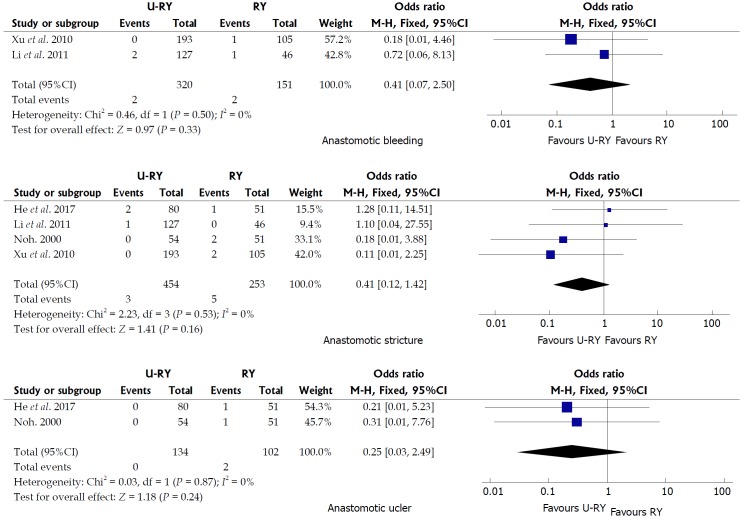
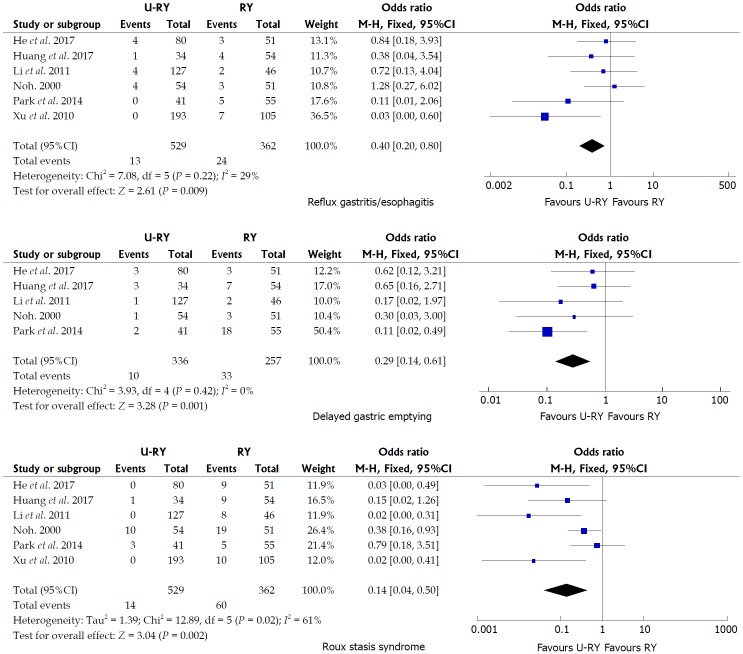
Methods: A literature search was conducted in Pubmed, Embase, Web of Science, Cochrane Library, Science Direct, Chinese National Knowledge Infrastructure, Wanfang, and China Science and Technology Journal Database to identify studies comparing U-RY with RY after DG for gastric cancer until the end of December 2017. Pooled odds ratio or weighted mean difference with 95% confidence interval was calculated using either fixed- or random-effects models. Perioperative outcomes such as operative time, intraoperative blood loss, and hospital stay; postoperative complications such as anastomotic bleeding, stricture and ulcer, reflux gastritis/esophagitis, delayed gastric emptying, and Roux stasis syndrome; and postoperative nutritional status (serum hemoglobin, total protein, and albumin levels) were the main outcomes assessed. Meta-analyses were performed using RevMan 5.3 software.
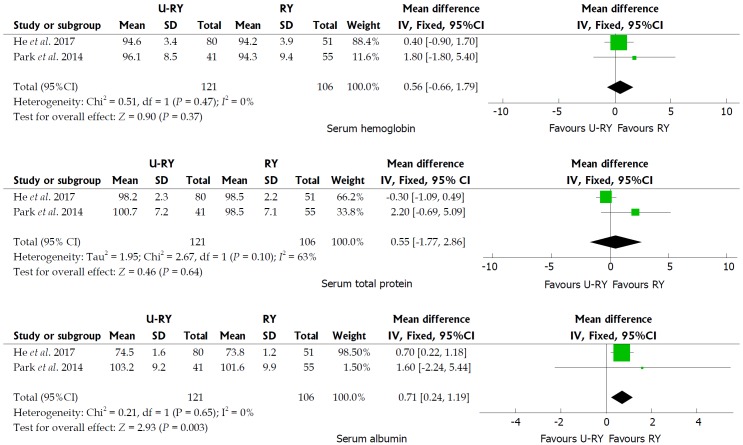
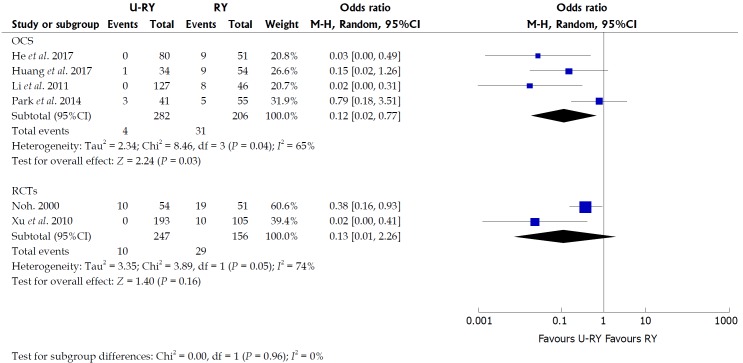
Results: Two randomized controlled trials and four nonrandomized observational clinical studies involving 403 and 488 patients, respectively, were included. The results of the meta-analysis showed that operative time [weighted mean difference (WMD): -12.95; 95%CI: -22.29 to -3.61; P = 0.007] and incidence of reflux gastritis/esophagitis (OR: 0.40; 95%CI: 0.20-0.80; P = 0.009), delayed gastric emptying (OR: 0.29; 95%CI: 0.14-0.61; P = 0.001), and Roux stasis syndrome (OR: 0.14; 95%CI: 0.04-0.50; P = 0.002) were reduced; and the level of serum albumin (WMD: 0.71; 95%CI: 0.24-1.19; P = 0.003) was increased in patients undergoing U-RY reconstruction compared with those undergoing RY reconstruction. No differences were found with respect to intraoperative blood loss, hospital stay, anastomotic bleeding, anastomotic stricture, anastomotic ulcer, the levels of serum hemoglobin, and serum total protein.
Conclusion: U-RY reconstruction has some clinical advantages over RY reconstruction after DG.
Keywords: Distal gastrectomy; Gastric cancer; Meta-analysis; Reconstruction; Roux-en-Y; Uncut.
Conflict of interest statement
Conflict-of-interest statement: The authors deny any conflict of interest.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Piessen G, Triboulet JP, Mariette C. Reconstruction after gastrectomy: which technique is best? J Visc Surg. 2010;147:e273–e283. - PubMed
-
- Hirao M, Takiguchi S, Imamura H, Yamamoto K, Kurokawa Y, Fujita J, Kobayashi K, Kimura Y, Mori M, Doki Y; Osaka University Clinical Research Group for Gastroenterological Study. Comparison of Billroth I and Roux-en-Y reconstruction after distal gastrectomy for gastric cancer: one-year postoperative effects assessed by a multi-institutional RCT. Ann Surg Oncol. 2013;20:1591–1597. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
