

Double Stimulation in the Same Ovarian Cycle (DuoStim) to Maximize the Number of Oocytes Retrieved From Poor Prognosis Patients: A Multicenter Experience and SWOT Analysis
- PMID: 29963011
- PMCID: PMC6010525
- DOI: 10.3389/fendo.2018.00317
Double Stimulation in the Same Ovarian Cycle (DuoStim) to Maximize the Number of Oocytes Retrieved From Poor Prognosis Patients: A Multicenter Experience and SWOT Analysis
Abstract
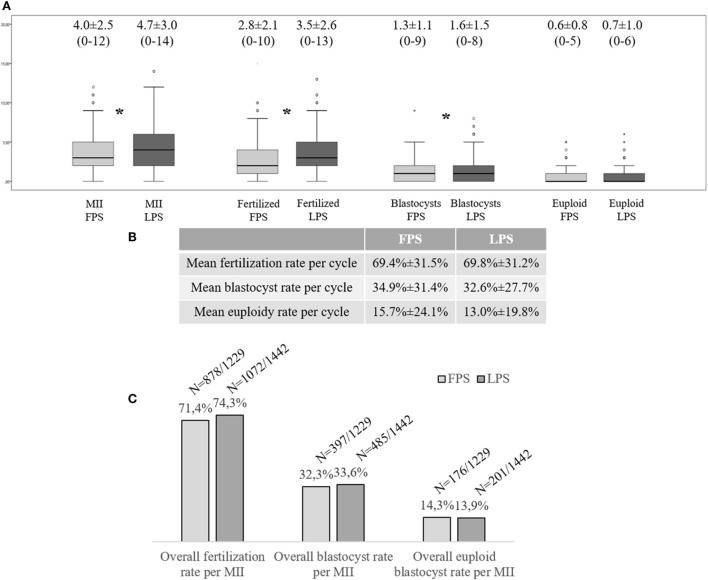
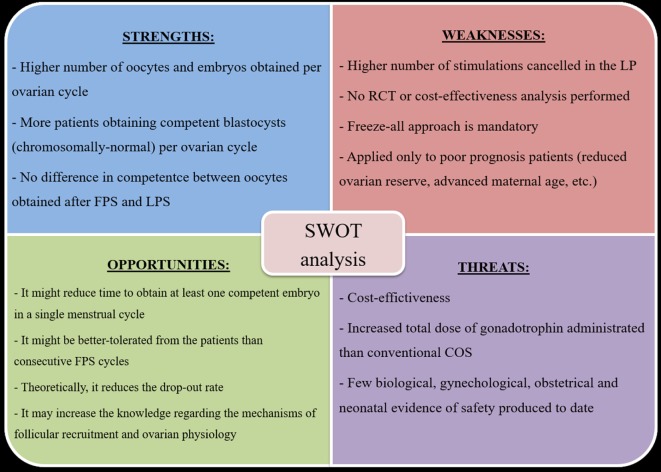
A panel of experts known as the POSEIDON group has recently redefined the spectrum of poor responder patients and introduced the concept of suboptimal response. Since an ideal management for these patients is still missing, they highlighted the importance of tailoring the ovarian stimulation based on the chance of each woman to obtain an euploid blastocyst. Interestingly, a novel pattern of follicle recruitment has been defined: multiple waves may arise during a single ovarian cycle. This evidence opened important clinical implications for the treatment of poor responders. For instance, double stimulation in the follicular (FPS) and luteal phase (LPS) of the same ovarian cycle (DuoStim) is an intriguing option to perform two oocyte retrievals in the shortest possible time. Here, we reported our 2-year experience of DuoStim application in four private IVF centers. To date, 310 poor prognosis patients completed a DuoStim protocol and underwent IVF with blastocyst-stage preimplantation-genetic-testing. LPS resulted into a higher mean number of oocytes collected than FPS; however, their competence (i.e., fertilization, blastocyst, euploidy rates, and clinical outcomes after euploid single-embryo-transfer) was comparable. Importantly, the rate of patients obtaining at least one euploid blastocyst increased from 42.3% (n = 131/310) after FPS to 65.5% (n = 203/310) with the contribution of LPS. A summary of the putative advantages and disadvantages of DuoStim was reported here through a Strengths-Weaknesses-Opportunities-Threats analysis. The strengths of this approach make it very promising. However, more studies are needed in the future to limit its weaknesses, shed light on its putative threats, and realize its opportunities.
Keywords: IVF; Poseidon; double stimulation; dual-stimulation; duostim; euploid blastocyst; low prognosis patients; poor responder.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous