Burden of Orofacial Clefting in India, 2016: A Global Burden of Disease Approach
- PMID: 29963432
- PMCID: PMC6018273
- DOI: 10.4103/ams.ams_196_17
Burden of Orofacial Clefting in India, 2016: A Global Burden of Disease Approach
Abstract
Background: In the recent past, there have been inconsistent reports of India witnessing a decreasing trend in the incidence of orofacial clefts (OFC). To date, little comprehensive evidence has been published. To identify the prevalence, associated burden in terms of epidemiological parameters and to estimate the "unmet" OFC treatment needs, the present study was undertaken.
Materials and methods: Using the Global Burden of Diseases 2016 approach and its assumptions, an attempt was made to estimate the prevalence to quantify the burden of OFC in India as disability-adjusted life years (DALYs), years of life lost (YLL), and years lived with disability (YLD) as well as death due to OFC. The results from such an approach are presented. Using previous estimates of "unmet" OFC treatment needs, an attempt was made to estimate the current volume of "unmet" OFC treatment needs.
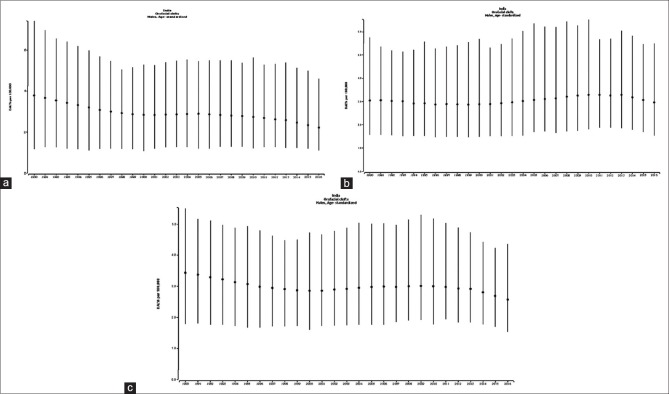
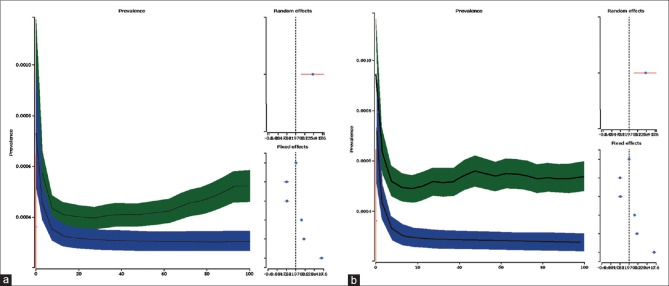
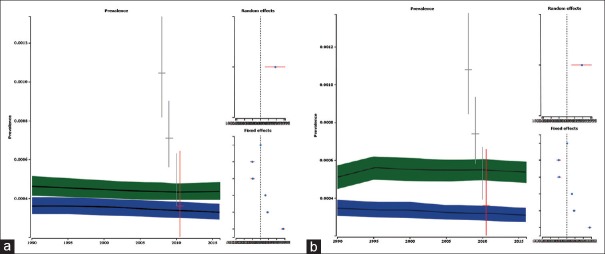
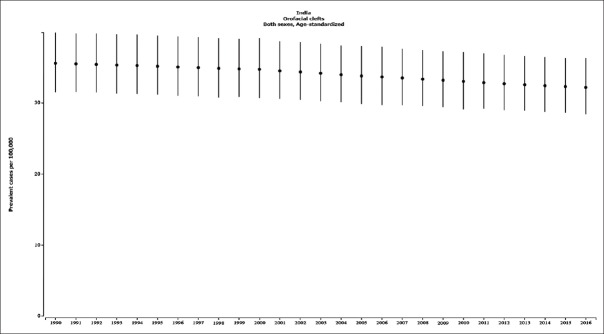
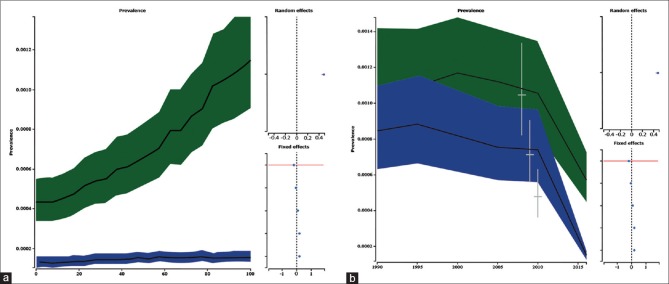
Results: In the present study, it was estimated that a total of 0.033% of all Indian population suffers from OFC. In 2016, the estimated prevalence rate/100,000 was 33.27 for males, 31.01 for females, and 32.18 combined for both genders. It was estimated that for all ages, the DALYs lost were 2.05 for 100,000 males, 2.66 for females and 2.34 for both sexes. The OFC birth prevalence model revealed that the birth prevalence (as a proportion) in 2016 in India showed an odds ratio of 0.48 (1.56-1.65) and fixed factor of nonrecording 0.83 (0.15-6.63), underreporting 0.97 (0.88-1), gender 1.09 (1.02-1.16), chromosomal diagnoses included 1.22 (1.22-1.22), and stillbirth 1.22 (1.22-1.22). The total unmet cleft treatment need was estimated at 79,430 or 18.76% of the total Indian cleft population with OFC.
Conclusions: Within the constraints of the mathematical modeling and based on all available surveys, literature, and reported data, the overall birth prevalence and the prevalence of OFC in India are presented. Till reliable data emerges, the present estimates could serve as a robust estimate of the prevalence and burden of OFC in India. The present enterprise highlights the need for well-designed, high-quality Pan-India, community-based, observational studies to accurately estimate the burden of OFC in India.
Keywords: Cleft lip; India; cleft palate; global burden of diseases; orofacial clefts.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Prevalence of orofacial clefts in Nigeria.Cleft Palate Craniofac J. 2014 May;51(3):320-5. doi: 10.1597/12-135. Epub 2013 Apr 4. Cleft Palate Craniofac J. 2014. PMID: 23557093 Free PMC article.
-
Prevalence and Patterns of Orofacial Clefts among Children from Different Regions of Saudi Arabia: A Systematic Review.Int J Clin Pediatr Dent. 2023 Jan-Feb;16(1):124-130. doi: 10.5005/jp-journals-10005-2507. Int J Clin Pediatr Dent. 2023. PMID: 37020763 Free PMC article. Review.
-
Disability adjusted life years for cancer patients in India.Asian Pac J Cancer Prev. 2010;11(3):633-40. Asian Pac J Cancer Prev. 2010. PMID: 21039029
-
Direct estimates of disability-adjusted life years lost due to stroke : a cross-sectional observational study in a demographic surveillance site in rural Gadchiroli, India.BMJ Open. 2019 Nov 7;9(11):e028695. doi: 10.1136/bmjopen-2018-028695. BMJ Open. 2019. PMID: 31699719 Free PMC article.
-
Global Prevalence and Burden of Orofacial Clefts: A Systematic Analysis for the Global Burden of Disease Study 2019.J Craniofac Surg. 2023 Oct 1;34(7):2012-2015. doi: 10.1097/SCS.0000000000009591. Epub 2023 Aug 15. J Craniofac Surg. 2023. PMID: 37582289 Free PMC article.
Cited by
-
Cleft Lip and Palate Research in Low- and Middle-income Countries: A Scientometric Analysis.Plast Reconstr Surg Glob Open. 2022 Feb 15;10(2):e4122. doi: 10.1097/GOX.0000000000004122. eCollection 2022 Feb. Plast Reconstr Surg Glob Open. 2022. PMID: 35186648 Free PMC article.
-
A Randomised Controlled Trial on the Effect of Hamulectomy on Hearing Outcomes in Cleft Palate Patients - A Comparative Study.Ann Maxillofac Surg. 2024 Jan-Jun;14(1):5-9. doi: 10.4103/ams.ams_185_23. Epub 2024 Apr 3. Ann Maxillofac Surg. 2024. PMID: 39184414 Free PMC article.
-
A Cross-Sectional Study: Are Myths on Cleft Lip and Palate Still Prevalent?Cureus. 2021 Nov 14;13(11):e19579. doi: 10.7759/cureus.19579. eCollection 2021 Nov. Cureus. 2021. PMID: 34926050 Free PMC article.
-
Reducing the burden of orthodontic care for children with clefts: evaluating the effectiveness of pre-alveolar bone graft orthodontics in unilateral non-syndromic cleft patients (PABO study)- A study protocol for a multicentric randomised controlled trial.Trials. 2021 Aug 28;22(1):572. doi: 10.1186/s13063-021-05505-0. Trials. 2021. PMID: 34454599 Free PMC article.
-
Gender inequality and burden of orofacial clefts in the Eastern Mediterranean region: findings from global burden of disease study 1990-2019.BMC Pediatr. 2024 Jan 23;24(1):76. doi: 10.1186/s12887-024-04569-6. BMC Pediatr. 2024. PMID: 38262976 Free PMC article.
References
-
- Mossey PA, Modell B. Epidemiology of oral clefts 2012: An international perspective. In: Cobourne MT, editor. Cleft Lip and Palate: Epidemiology, Aetiology and Treatment. Front Oral Biology. Vol. 16. Basel: Karger; 2012. pp. 1–18. - PubMed
-
- Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet. 2009;374:1773–85. - PubMed
-
- Patil SB, Kale SM, Khare N, Math M, Jaiswal S, Jain A, et al. Changing patterns in demography of cleft lip-cleft palate deformities in a developing country: The smile train effect – What lies ahead? Plast Reconstr Surg. 2011;127:327–32. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous