Recurrent symptomatic cemento-osseous dysplasia: A case report
- PMID: 29963485
- PMCID: PMC6015922
- DOI: 10.5624/isd.2018.48.2.131
Recurrent symptomatic cemento-osseous dysplasia: A case report
Abstract
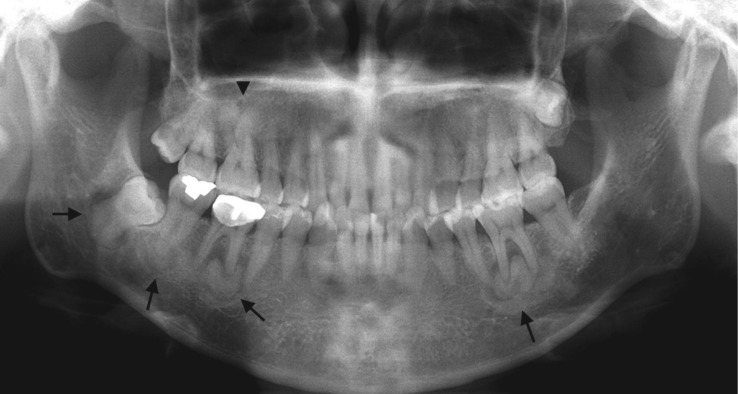
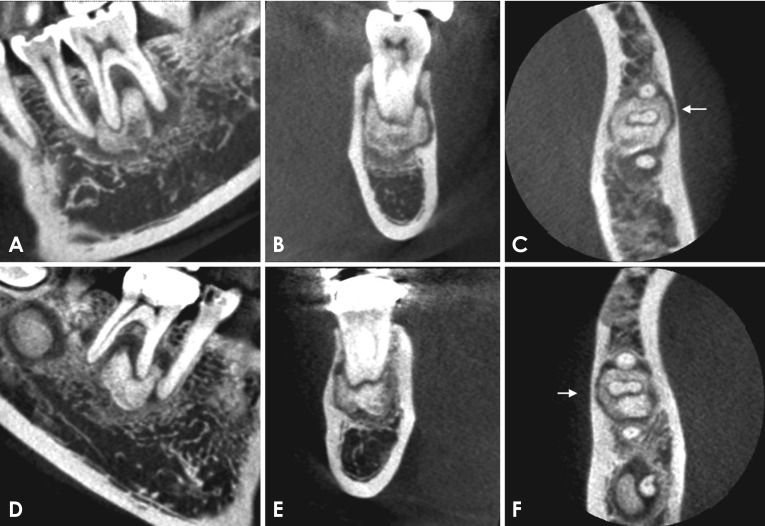
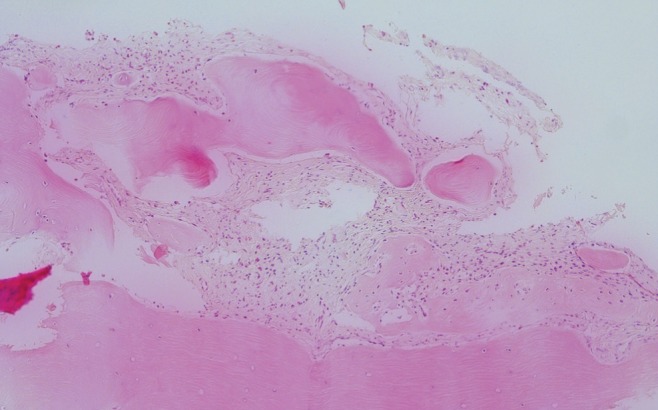
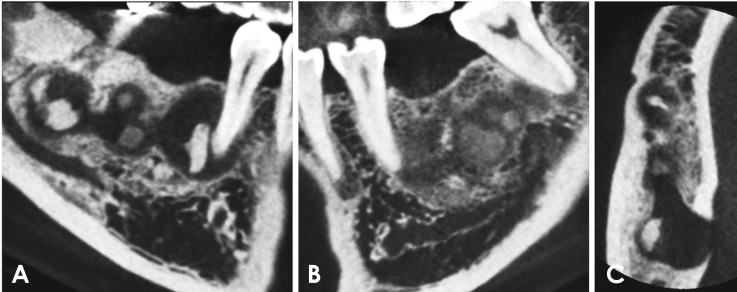
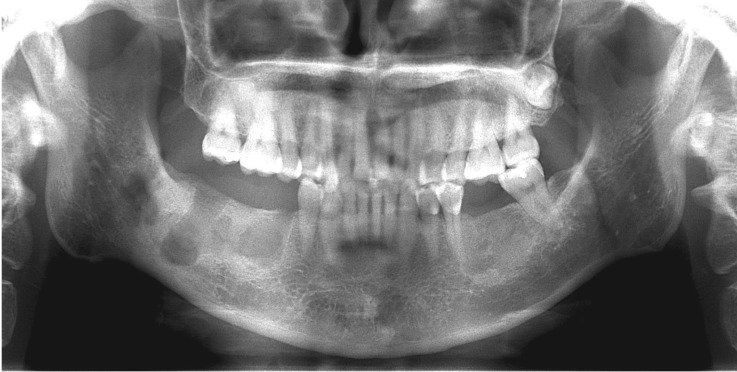
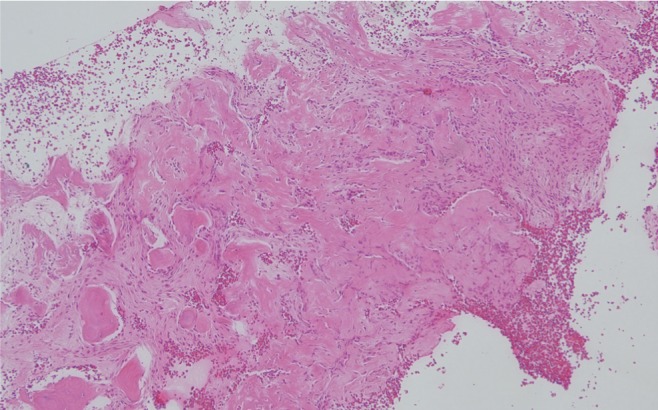
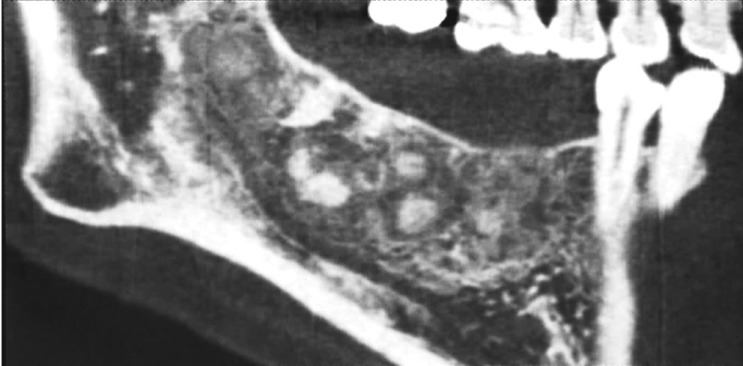
Cemento-osseous dysplasia (COD) is a benign fibro-osseous lesion of bone, in which normal bone is replaced by fibrous tissue, followed by calcification with osseous and cementum-like tissue. COD is classified into 3 categories according to its location: periapical, focal, and florid COD (FCOD). On radiography, FCOD appears radiolucent in its early stages. As it matures, radiopacities appear within the lesion, causing them to show a mixed appearance of radiolucency and radiopacity. Because FCOD is usually asymptomatic and grows in a self-limited manner, it does not require treatment. Secondary infection is the most frequent cause of symptomatic cases. We report a case of FCOD with symptoms that appeared after a dental restoration procedure and persisted after repeated operations. The purpose of this report is to emphasize the importance of thorough radiological evaluations of patients with FCOD before treatment.
Keywords: Bone Diseases; Cone-Beam Computed Tomography; Florid Cemento-osseous Dysplasia; Radiography, Panoramic.
Figures


References
-
- MacDonald DS. Maxillofacial fibro-osseous lesions. Clin Radiol. 2015;70:25–36. - PubMed
-
- MacDonald-Jankowski DS. Florid cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2003;32:141–149. - PubMed
-
- Mainville GN, Turgeon DP, Kauzman A. Diagnosis and management of benign fibro-osseous lesions of the jaws: a current review for the dental clinician. Oral Dis. 2017;23:440–450. - PubMed
-
- Su L, Weathers DR, Waldron CA. Distinguishing features of focal cemento-osseous dysplasia and cemento-ossifying fibromas. II. A clinical and radiologic spectrum of 316 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:540–549. - PubMed
-
- Cavalcanti PH, Nascimento EH, Pontual ML, Pontual AD, Marcelos PG, Perez DE, et al. Cemento-osseous dysplasias: imaging features based on cone beam computed tomography scans. Braz Dent J. 2018;29:99–104. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials