Maxillofacial reconstruction with Medpor porous polyethylene implant: a case series study
- PMID: 29963494
- PMCID: PMC6024064
- DOI: 10.5125/jkaoms.2018.44.3.128
Maxillofacial reconstruction with Medpor porous polyethylene implant: a case series study
Abstract
Objectives: The role of alloplastic materials in maxillofacial reconstruction is still controversial. Determining the utility of porous, high-density, polyethylene implants as a highly stable and flexible, porous alloplast, with properties such as rapid vascularization and tissue ingrowth, is crucial in cases of maxillofacial deformities and aesthetic surgery.
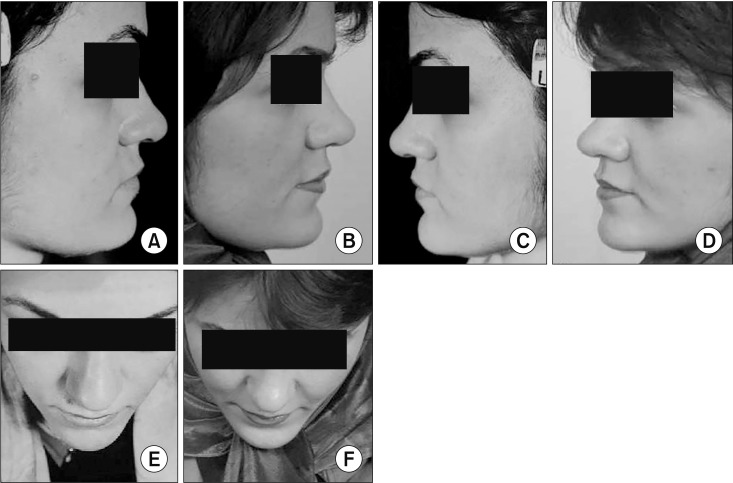
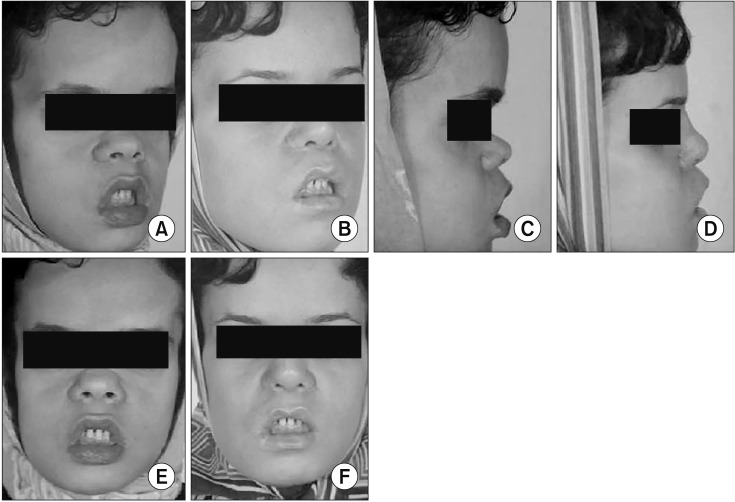
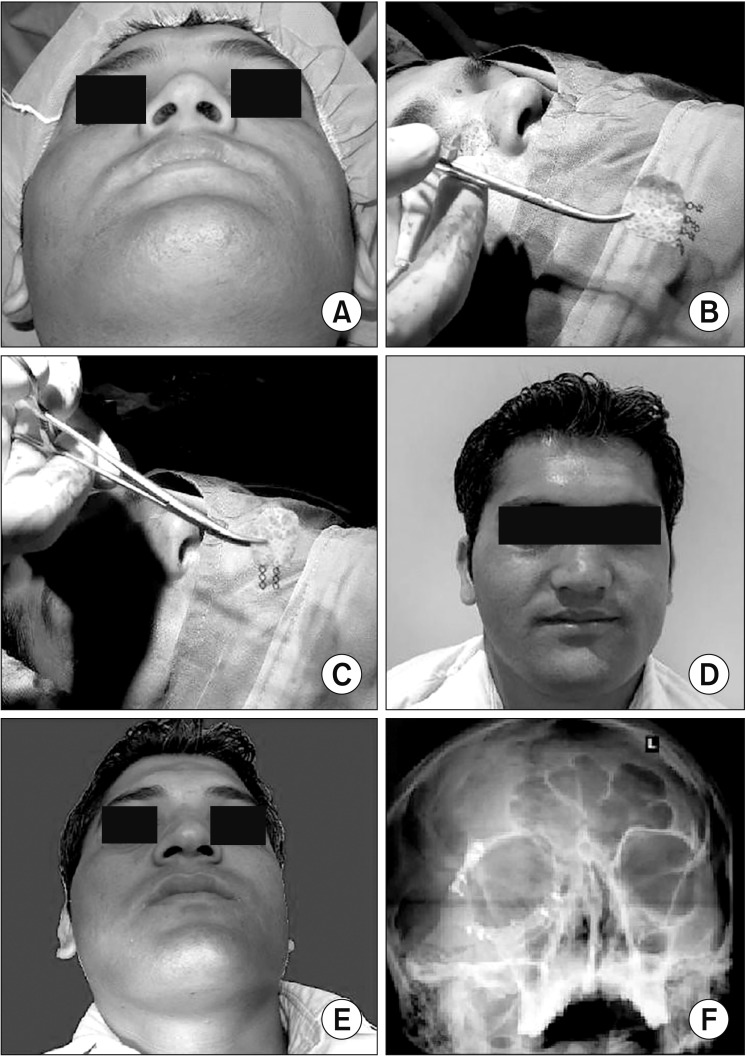
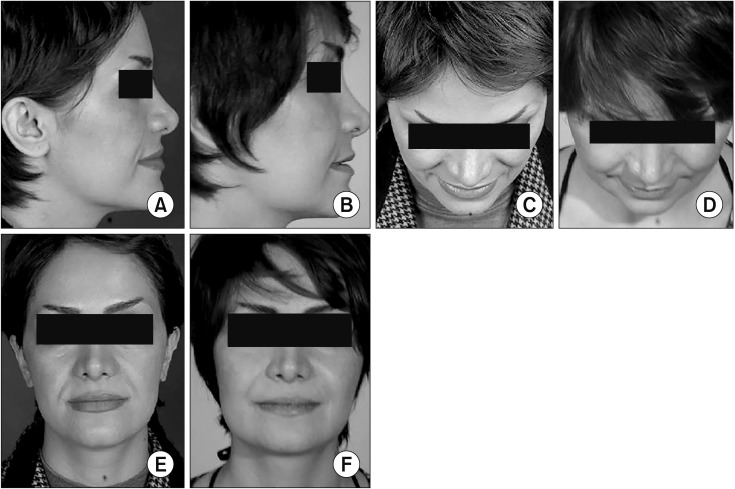
Materials and methods: Thirty high-density porous polyethylene implants were implanted in 16 patients that had been referred to a private office over a three-year period. These implants were used for correcting congenital deformities, posttraumatic defects and improving the aesthetic in nasal, paranasal, malar, chin, mandibular angle, body and orbital areas.
Results: The outcomes of the cases in this study showed good aesthetic and functional results. The majority of patients had no signs of discomfort, rejection or exposure. Two implants suffered complications: a complicated malar implant was managed by antibiotic therapy, and an infected mandibular angle implant was removed despite antibiotic therapy.
Conclusion: Based on the results, the Medpor implant seems to be an excellent biomaterial for correcting various facial deformities. Advantages include its versatility and relatively ideal pore size that allows for excellent soft tissue ingrowth and coverage. It is strong, flexible and easy to shape.
Keywords: Maxillofacial prosthesis implantation; Medpor; Reconstructive surgical procedures.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Rees TD. Physical considerations for the aesthetic surgery of the neck and face. In: Rees TD, editor. Aesthetic plastic surgery. Philadelphia: W.B. Saunders; 1980. p. 587.
-
- Maas CS, Merwin GE, Wilson J, Frey MD, Maves MD. Comparison of biomaterials for facial bone augmentation. Arch Otolaryngol Head Neck Surg. 1990;116:551–556. - PubMed
-
- Wolfe SA, Berkowitz S. Plastic surgery of the facial skeleton. Boston: Little, Brown; 1989. p. 687.
-
- Spector M, Harmon SL, Kreutner A. Characteristics of tissue growth into proplast and porous polyethylene implants in bone. J Biomed Mater Res. 1979;13:677–692. - PubMed
-
- Breadon GE, Kern EB, Neel HB., 3rd Autografts of uncrushed and crushed bone and cartilage. Experimental observations and clinical implications. Arch Otolaryngol. 1979;105:75–80. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources