

Estimating relative efficacy in acute postoperative pain: network meta-analysis is consistent with indirect comparison to placebo alone
- PMID: 29965830
- PMCID: PMC6203421
- DOI: 10.1097/j.pain.0000000000001322
Estimating relative efficacy in acute postoperative pain: network meta-analysis is consistent with indirect comparison to placebo alone
Abstract
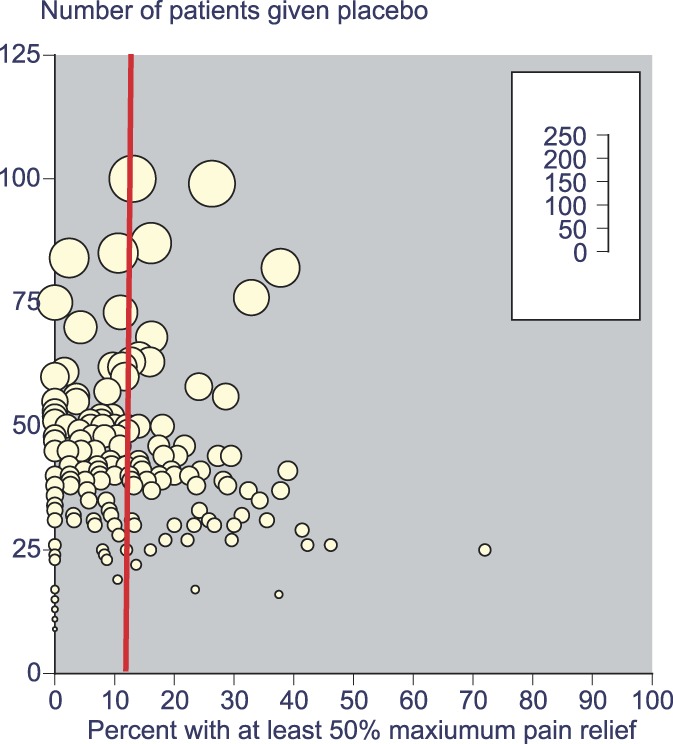
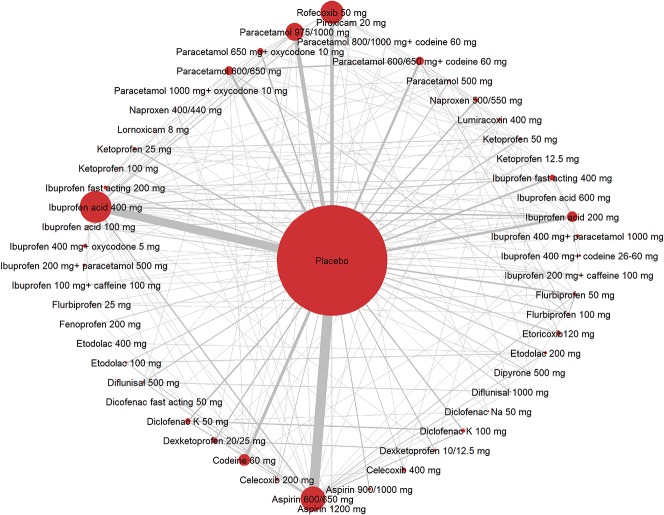
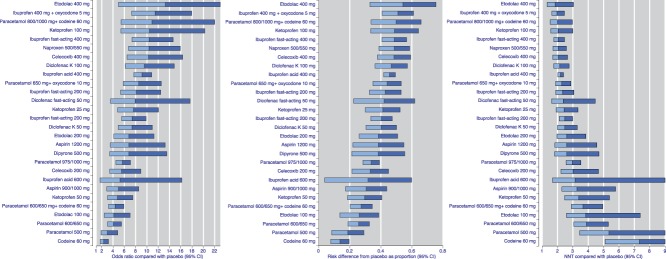
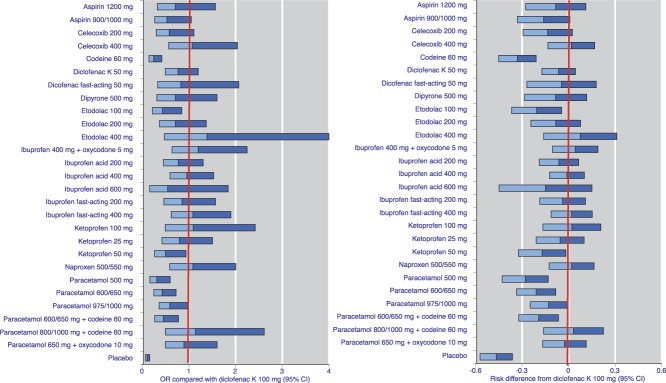
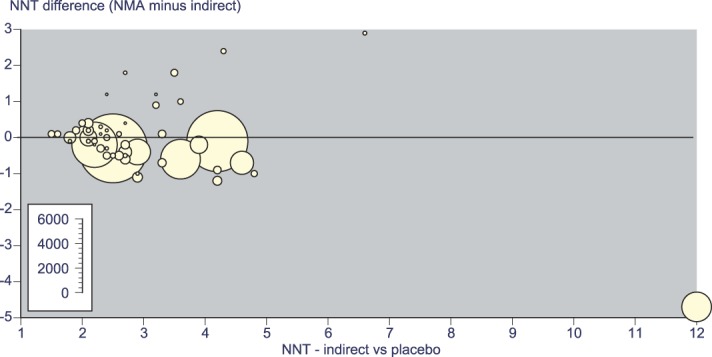
Network meta-analysis uses direct comparisons of interventions within randomized controlled trials and indirect comparisons across them. Network meta-analysis uses more data than a series of direct comparisons with placebo, and theoretically should produce more reliable results. We used a Cochrane overview review of acute postoperative pain trials and other systematic reviews to provide data to test this hypothesis. Some 261 trials published between 1966 and 2016 included 39,753 patients examining 52 active drug and dose combinations (27,726 given active drug and 12,027 placebo), in any type of surgery (72% dental). Most trials were small; 42% of patients were in trials with arms <50 patients, and 27% in trials with arms ≥100 patients. Response to placebo in third molar extraction fell by half in studies over 30 to 40 years (171 trials, 7882 patients given placebo). Network meta-analysis and Cochrane analyses provided very similar results (average difference 0.04 number needed to treat units), with no significant difference for almost all comparisons apart from some with small patient numbers or small effect size, or both. Network meta-analysis did not detect significant differences between effective analgesics. The similarity between network meta-analysis and Cochrane indirect analyses probably arose from stringent quality criteria in trials accepted in Cochrane reviews (with consequent low risk of bias) and consistency in methods and outcomes. Network meta-analysis is a useful analytical tool that increases our confidence in estimates of efficacy of analgesics in acute postoperative pain, in this case by providing similar results.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures

References
-
- AlBalawi Z, McAlister FA, Thorlund K, Wong M, Wetterslev J. Random error in cardiovascular meta-analyses: how common are false positive and false negative results? Int J Cardiol 2013;168:1102–7. - PubMed
-
- Barden J, Derry S, McQuay HJ, Moore RA. Bias from industry trial funding? A framework, a suggested approach, and a negative result. PAIN 2006;121:207–18. - PubMed
-
- Barden J, Edwards JE, McQuay HJ, Andrew Moore R. Pain and analgesic response after third molar extraction and other postsurgical pain. PAIN 2004;107:86–90. - PubMed
-
- Collins SL, Edwards J, Moore RA, Smith LA, McQuay HJ. Seeking a simple measure of analgesia for mega-trials: is a single global assessment good enough? PAIN 2001;91:189–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
