

Pacing for Vasovagal Syncope
- PMID: 29967681
- PMCID: PMC6020179
- DOI: 10.15420/aer.2018.22.2
Pacing for Vasovagal Syncope
Abstract
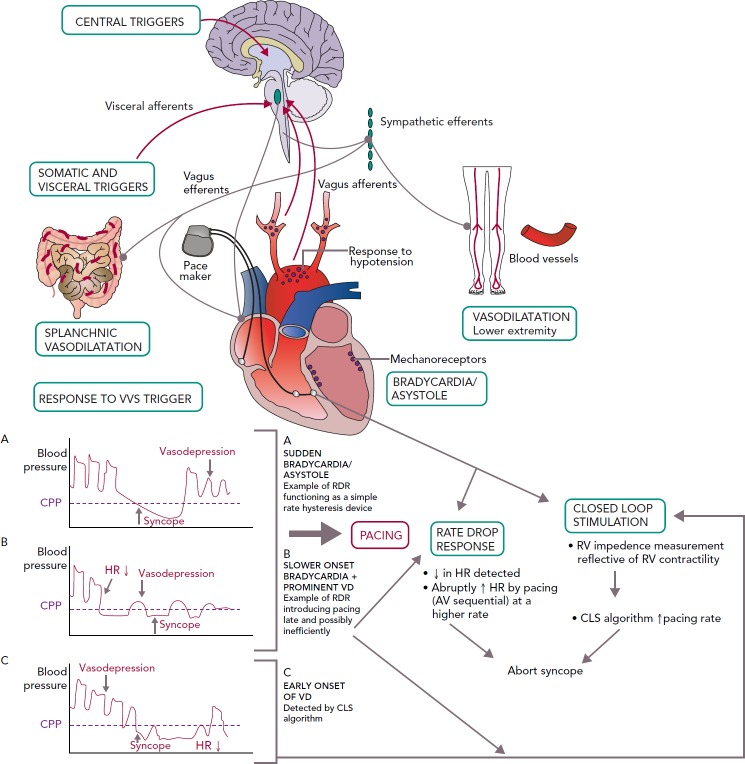
Vasovagal syncope (VVS) is due to a common autonomic reflex involving the cardiovascular system. It is associated with bradycardia (cardioinhibitory response) and/or hypotension (vasodepressor response), likely mediated by parasympathetic activation and sympathetic inhibition. While generally a situational, isolated and/or self-limited event, for some, VVS is recurrent, unpredictable and debilitating. Conservative, non-pharmacological management may help, but no specific medical therapy has been proven widely effective. Permanent pacing may have specific benefit, but its value has been debated. The temporal causative association of bradycardia with syncope in those with VVS may help identify which patient could benefit from pacing but the timing and type of pacing in lieu of blood pressure changes may be critical. The mode, rate, pacing algorithm and time to initiate dual-chamber pacing preferentially with respect to the vasovagal reflex may be important to prevent or ameliorate the faint but completely convincing data are not yet available. Based on available data, DDD pacing with the closed loop stimulation algorithm appears a viable, if not the best, alternative presently to prevent recurrent VVS episodes. While several knowledge gaps remain, permanent pacing appears to have a role in managing select patients with VVS.
Keywords: Syncope; asystole; closed loop stimulation; pacing; rate drop response; vasovagal syncope.
Conflict of interest statement
Disclosure: Rakesh Gopinathannair has received consultant/speaker fees from Abbott, the American Heart Association, Pfizer, Bristol Myers Squibb and Zoll, and is on the advisory board of HealthTrust PG. Brian Olshansky has received consultant/speaker fees from Amarin Corporation, Boehringer Ingelheim, Cryolife and Lundbeck. Benjamin Salgado has no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
