

Perioperative serum cortisol levels in ACTH sufficient and ACTH deficient patients during transsphenoidal surgery of pituitary adenoma
- PMID: 29968225
- PMCID: PMC6153577
- DOI: 10.1007/s12020-018-1655-8
Perioperative serum cortisol levels in ACTH sufficient and ACTH deficient patients during transsphenoidal surgery of pituitary adenoma
Abstract
Purpose: No previous study has analyzed serum cortisol levels during transsphenoidal endoscopic pituitary surgery in patients with and without hydrocortisone (HC) substitution.
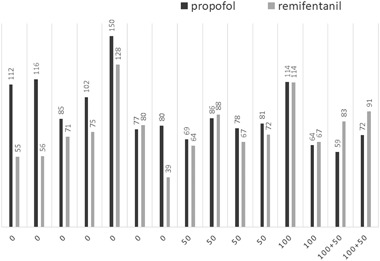
Methods: A total of 15 patients undergoing surgery for a pituitary adenoma were studied. Those with normal ACTH function were either not given HC (n = 7) or received 50 mg intravenous HC at the start of surgery (n = 4). Patients with ACTH deficiency received intravenous HC of 100 mg in the morning before surgery (n = 4) with the additional 50 mg for an afternoon operation (n = 2). Propofol and remifentanil were used as anesthetics. Serum cortisol was measured at the start of and every 30 min during surgery.
Results: Among 7 patients with normal ACTH function without HC substitution, cortisol levels before surgery were 126-244 nmol/L, among the 4 patients undergoing surgery in the morning, whereas the 3 who underwent surgery in the afternoon had lower levels, 38-76 nmol/L. During nose/sinus surgery cortisol levels decreased to 79-139 and 24-54 nmol/L, respectively. At intrasellar manipulation a distinct rise was noted. Also, in the 4 ACTH sufficient patients receiving HC, cortisol levels decreased during nose/sinus surgery, but only with a slight increase during intrasellar surgery. In the 4 ACTH deficient patients cortisol peaked at 1914-2582 nmol/L.
Conclusions: Patients with normal ACTH function without HC substitution had very low cortisol levels during the first part of surgery, likely suppressed by the anesthetics. After mechanical impact in the sella, a marked increase in cortisol was noted. Supraphysiological cortisol levels were achieved with our routine HC substitution, advising us to reduce the supplementation.
Keywords: Hydrocortisone; adrenal insufficiency; pituitary gland; adrenocorticotropic hormone; endoscopic transsphenoidal surgery; remifentanil.
Conflict of interest statement
Conflict of interest
Eva Marie Erfurth received lecture fees from Pfizer and Eli Lilly. The other authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the ethics committee of Lund University, Sweden (2012/374). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures


Similar articles
-
Early morning cortisol levels as predictors of short-term and long-term adrenal function after endonasal transsphenoidal surgery for pituitary adenomas and Rathke's cleft cysts.World Neurosurg. 2013 Nov;80(5):569-75. doi: 10.1016/j.wneu.2012.07.034. Epub 2012 Aug 14. World Neurosurg. 2013. PMID: 22902358
-
Which patients benefit from provocative adrenal testing after transsphenoidal pituitary surgery?Clin Endocrinol (Oxf). 1997 Jan;46(1):21-7. doi: 10.1046/j.1365-2265.1997.d01-1748.x. Clin Endocrinol (Oxf). 1997. PMID: 9059554
-
Consensus-driven in-hospital cortisol assessment after ACTH-secreting pituitary adenoma resection.Pituitary. 2018 Feb;21(1):41-49. doi: 10.1007/s11102-017-0845-3. Pituitary. 2018. PMID: 29143885
-
Endoscopic Endonasal Surgery for Remission of Cushing Disease Caused by Ectopic Intracavernous Macroadenoma: Case Report and Literature Review.World Neurosurg. 2017 Feb;98:870.e5-870.e10. doi: 10.1016/j.wneu.2016.12.021. Epub 2016 Dec 18. World Neurosurg. 2017. PMID: 28003168 Review.
-
Cushing disease: use of perioperative serum cortisol measurements in early determination of success following pituitary surgery.Neurosurg Focus. 2007;23(3):E6. doi: 10.3171/foc.2007.23.3.8. Neurosurg Focus. 2007. PMID: 17961022 Review.
Cited by
-
Perioperative Outcomes of a Hydrocortisone Protocol after Endonasal Surgery for Pituitary Adenoma Resection.J Neurol Surg B Skull Base. 2021 Sep 27;83(4):383-389. doi: 10.1055/s-0041-1735588. eCollection 2022 Aug. J Neurol Surg B Skull Base. 2021. PMID: 35903648 Free PMC article.
-
Evaluation of different hydrocortisone treatment strategies in transsphenoidal pituitary surgery.Acta Neurochir (Wien). 2019 Aug;161(8):1715-1721. doi: 10.1007/s00701-019-03885-6. Epub 2019 May 7. Acta Neurochir (Wien). 2019. PMID: 31065892 Free PMC article.
-
Investigation of the Hypothalamo-pituitary-adrenal (HPA) axis: a contemporary synthesis.Rev Endocr Metab Disord. 2021 Jun;22(2):179-204. doi: 10.1007/s11154-020-09611-3. Epub 2021 Mar 26. Rev Endocr Metab Disord. 2021. PMID: 33770352 Review.
-
Prospective Evaluation of Transsphenoidal Pituitary Surgery in Patients with Cushing's Disease: Delayed Remission and the Role of Postsurgical Cortisol as a Predictive Factor.Healthcare (Basel). 2024 Sep 22;12(18):1900. doi: 10.3390/healthcare12181900. Healthcare (Basel). 2024. PMID: 39337241 Free PMC article.
-
Safety of Withholding Perioperative Hydrocortisone for Patients With Pituitary Adenomas With an Intact Hypothalamus-Pituitary-Adrenal Axis: A Randomized Clinical Trial.JAMA Netw Open. 2022 Nov 1;5(11):e2242221. doi: 10.1001/jamanetworkopen.2022.42221. JAMA Netw Open. 2022. PMID: 36383383 Free PMC article. Clinical Trial.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
