

Extensive clinical experience: Hypothalamic-pituitary-adrenal axis recovery after adrenalectomy for corticotropin-independent cortisol excess
- PMID: 29968420
- PMCID: PMC6246804
- DOI: 10.1111/cen.13803
Extensive clinical experience: Hypothalamic-pituitary-adrenal axis recovery after adrenalectomy for corticotropin-independent cortisol excess
Abstract
Objective: To identify predictors of hypothalamic-pituitary-adrenal (HPA) axis recovery interval and severity of glucocorticoid withdrawal symptoms (GWS) in patients undergoing adrenalectomy for corticotropin-independent cortisol excess.
Design: This is a retrospective study of patients with mild autonomous cortisol excess (MACE), moderate and severe Cushing syndrome (CS) who developed adrenal insufficiency after unilateral adrenalectomy between 1998 and 2017.
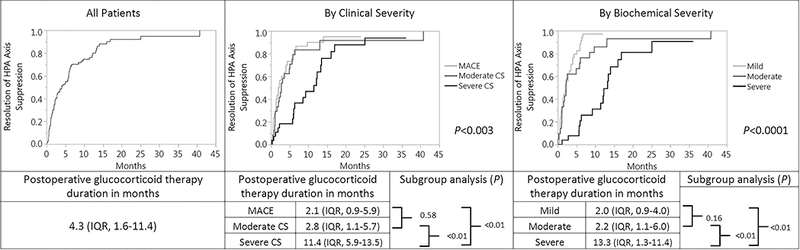
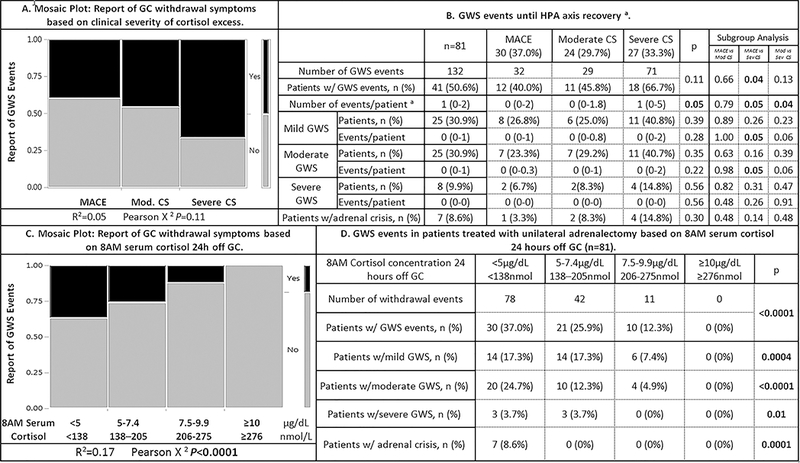
Results: Adrenalectomy was performed in 81 patients (79% women, median age 52 years [IQR 42-62]). HPA axis recovery occurred at a median of 4.3 months (IQR 1.6-11.4) after adrenalectomy (severe CS vs moderate CS vs MACE: median 11.4 vs 2.8 vs 2.1 months, P < 0.01). Main predictors of HPA axis recovery interval included: preoperative serum cortisol concentration after 1-mg overnight dexamethasone suppression test >10 μg/dL or >276 nmol/L (9.7 vs 1.3 months if cortisol ≤10 μg/dL or ≤276 nmol/L, P < 0.01); body mass index (for every 3 kg/m2 decrease, glucocorticoid taper increased by 1 month, P < 0.05); age <45 (11.4 vs 2.3 months if ≥45 years, P < 0.05); duration of symptoms prior to diagnosis >1 year (11.4 vs 2.8 months if ≤1 year); moon facies (11.4 vs 2.2 months if no rounding of the face); and myopathy (13.1 vs 2.7 months if no myopathy, P < 0.05). Patients with severe CS had a higher incidence of GWS compared to patients with MACE (66.7% vs 40.0%, P < 0.05) with a median of 1 and 0 events/patient, respectively.
Conclusions: The HPA axis recovery interval was the longest for patients with severe CS. Surprisingly, patients with moderate CS recovered their HPA axis as quickly as those with MACE. Glucocorticoid withdrawal symptoms were observed in all groups, with more events in patients with severe CS. This study emphasizes the need to counsel patients on expectations for HPA axis recovery and address intervention for GWS based on individual preoperative parameters.
Keywords: ACTH-independent Cushing syndrome; adrenal insufficiency; adrenalectomy; adrenocortical hyperfunction; glucocorticoids; hypothalamic-pituitary-adrenal axis; pituitary-adrenal system; substance withdrawal syndrome.
© 2018 John Wiley & Sons Ltd.
Figures
Comment in
-
Management of glucocorticoids following adrenalectomy for ACTH-independent Cushing's syndrome.Clin Endocrinol (Oxf). 2018 Dec;89(6):719-720. doi: 10.1111/cen.13839. Epub 2018 Sep 13. Clin Endocrinol (Oxf). 2018. PMID: 30129044 No abstract available.
References
-
- Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol . 2016;175(2):G1–g34. - PubMed
-
- Bancos I, Alahdab F, Crowley RK, et al. THERAPY OF ENDOCRINE DISEASE: Improvement of cardiovascular risk factors after adrenalectomy in patients with adrenal tumors and subclinical Cushing’s syndrome: a systematic review and meta-analysis. Eur J Endocrinol . 2016;175(6):R283–r295. - PubMed
-
- Di Dalmazi G, Vicennati V, Garelli S, et al. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing’s syndrome: a 15-year retrospective study. Lancet Diabetes Endocrinol . 2014;2(5):396–405. - PubMed
-
- Clayton RN, Jones PW, Reulen RC, et al. Mortality in patients with Cushing’s disease more than 10 years after remission: a multicentre, multinational, retrospective cohort study. The lancet Diabetes & endocrinology . 2016;4(7):569–576. - PubMed
-
- Morelli V, Palmieri S, Salcuni AS, et al. Bilateral and unilateral adrenal incidentalomas: biochemical and clinical characteristics. Eur J Endocrinol . 2013;168(2):235–241. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
