

The Evolving Concept of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention: Focus on Unique Feature of East Asian and "Asian Paradox"
- PMID: 29968428
- PMCID: PMC6031716
- DOI: 10.4070/kcj.2018.0166
The Evolving Concept of Dual Antiplatelet Therapy after Percutaneous Coronary Intervention: Focus on Unique Feature of East Asian and "Asian Paradox"
Abstract
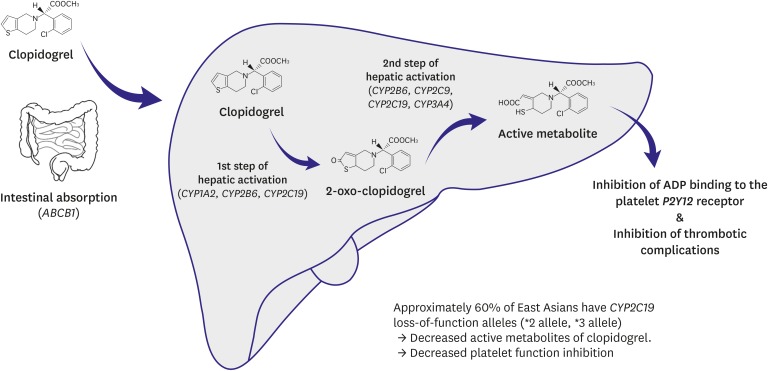
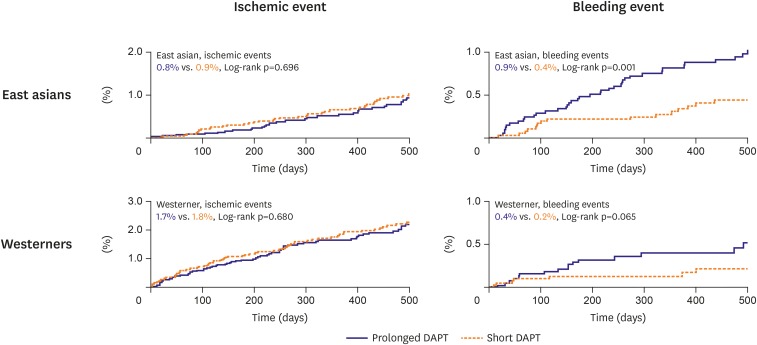
Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor is essential after percutaneous coronary intervention (PCI), while many studies have focused on determining the optimal degree of platelet inhibition and optimal DAPT duration to minimize complications after PCI. Current guidelines developed by the American College of Cardiology/American Heart Association and the European Society of Cardiology summarize previous studies and provide recommendations. However, these guidelines are mainly based on Western patients, and their characteristics might differ from those of East Asian patients. Previous data suggested that East Asian patients have unique features with regard to the response to antiplatelet agents. On comparing Western and East Asian patients, it was found that East Asian patients have a lower rate of ischemic events and higher rate of bleeding events after PCI, despite a higher on-treatment platelet reactivity, which is referred to as the "East Asian paradox." As the main purpose of DAPT is to minimize ischemic and bleeding complications after PCI, these differences should be clarified before adopting the guidelines for East Asian patients. Therefore, in this article, we will review various issues regarding DAPT in East Asian patients, with a focus on the unique characteristics of East Asian patients, previous studies regarding antiplatelet agents in East Asian patients, and a guideline from an East Asian perspective.
Keywords: Bleeding risk; Dual antiplatelet therapy; East Asians; Ischemic risk; Percutaneous coronary intervention.
Copyright © 2018. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Schömig A, Neumann FJ, Kastrati A, et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med. 1996;334:1084–1089. - PubMed
-
- Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH CLASSICS Investigators. Double-blind study of the safety of clopidogrel with and without a loading dose in combination with aspirin compared with ticlopidine in combination with aspirin after coronary stenting: the clopidogrel aspirin stent international cooperative study (CLASSICS) Circulation. 2000;102:624–629. - PubMed
-
- Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:1706–1717. - PubMed
-
- Steinhubl SR, Berger PB, Mann JT, 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288:2411–2420. - PubMed
-
- Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Kardiol Pol. 2017;75:1217–1299. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
