

Metronomic capecitabine vs. best supportive care in Child-Pugh B hepatocellular carcinoma: a proof of concept
- PMID: 29968763
- PMCID: PMC6030080
- DOI: 10.1038/s41598-018-28337-6
Metronomic capecitabine vs. best supportive care in Child-Pugh B hepatocellular carcinoma: a proof of concept
Abstract
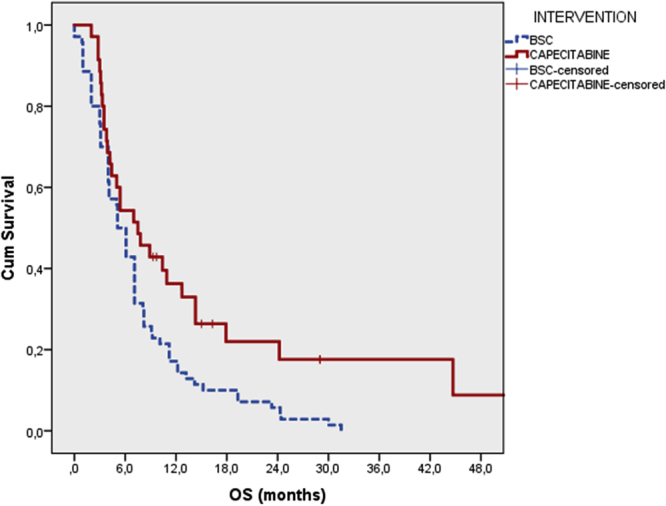
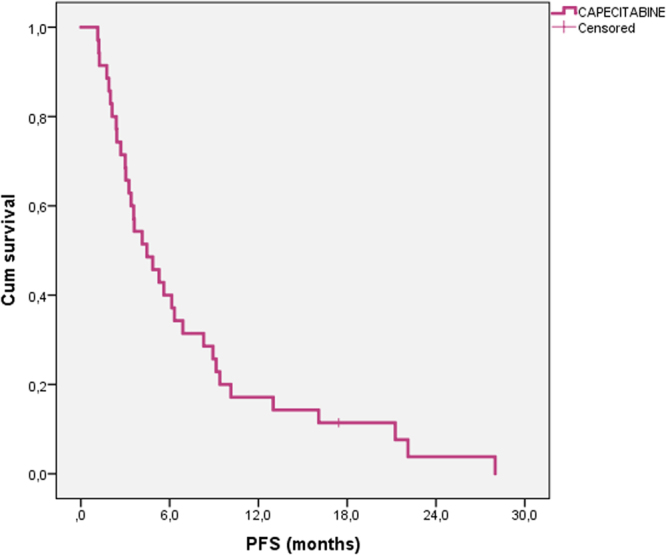
There is a relative lack of evidence about systemic treatments in patients with hepatocellular carcinoma (HCC) and moderate liver dysfunction (Child-Pugh B). In this multicenter study we retrospectively analyzed data from Child-Pugh B-HCC patients naïve to systemic therapies, treated with MC or best supportive care (BSC). To reduce the risk of selection bias, an inverse probability of treatment weighting approach was adopted. Propensity score was generated including: extrahepatic spread; macrovascular invasion; performance status, alphafetoprotein > 400 ng/ml, Child- Pugh score [B7 vs. B8-9]. We identified 35 MC-treated patients and 70 controls. Median overall survival was 7.5 [95% CI: 3.733-11.267]in MC-patients and 5.1 months [95% CI: 4.098-6.102] in the BSC group (p = 0.013). In patients treated with MC, median progression-free survival was 4.5 months (95% CI: 2.5-6.5). The univariate unweighted Cox regression showed a 42% reduction in death risk for patients on MC (95%CI: 0.370-0.906; p = 0.017). After weighting for potential confounders, death risk remained essentially unaltered. In the MC group, 12 patients (34.3%) experienced at least one adverse event, the most common of which were: fatigue (17.1%), hand-foot syndrome (8.5%), thrombocytopenia (8.5%), and neutropenia (5.7%). MC seems a safe option for Child-Pugh B-HCC patients. Its potential antitumour activity warrants prospective evaluations.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Sorafenib and Metronomic Capecitabine in Child-Pugh B patients with advanced HCC: A real-life comparison with best supportive care.Dig Liver Dis. 2024 Sep;56(9):1582-1591. doi: 10.1016/j.dld.2024.01.199. Epub 2024 Feb 9. Dig Liver Dis. 2024. PMID: 38341377
-
Metronomic capecitabine versus best supportive care as second-line treatment in hepatocellular carcinoma: a retrospective study.Sci Rep. 2017 Feb 13;7:42499. doi: 10.1038/srep42499. Sci Rep. 2017. PMID: 28211921 Free PMC article.
-
The power of kindness: curative treatment with metronomic combination in advanced hepatocellular carcinoma.Anticancer Drugs. 2022 Jan 1;33(1):e781-e783. doi: 10.1097/CAD.0000000000001202. Anticancer Drugs. 2022. PMID: 34407053
-
Treatment of hepatocellular carcinoma in Child-Pugh B patients.Dig Liver Dis. 2013 Oct;45(10):852-8. doi: 10.1016/j.dld.2013.03.002. Epub 2013 Apr 9. Dig Liver Dis. 2013. PMID: 23582346
-
Capecitabine in advanced hepatocellular carcinoma: A multicenter experience.Dig Liver Dis. 2019 Dec;51(12):1713-1719. doi: 10.1016/j.dld.2019.06.015. Epub 2019 Jul 16. Dig Liver Dis. 2019. PMID: 31320302
Cited by
-
Recent Update on Immunotherapy and Its Combination With Interventional Therapies for Hepatocellular Carcinoma.Clin Med Insights Oncol. 2022 Nov 11;16:11795549221134832. doi: 10.1177/11795549221134832. eCollection 2022. Clin Med Insights Oncol. 2022. PMID: 36387611 Free PMC article. Review.
-
Understanding the Immunoenvironment of Primary Liver Cancer: A Histopathology Perspective.J Hepatocell Carcinoma. 2022 Nov 2;9:1149-1169. doi: 10.2147/JHC.S382310. eCollection 2022. J Hepatocell Carcinoma. 2022. PMID: 36349146 Free PMC article. Review.
-
Efficacy and safety of atezolizumab plus bevacizumab combined with hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma.Front Immunol. 2022 Aug 5;13:929141. doi: 10.3389/fimmu.2022.929141. eCollection 2022. Front Immunol. 2022. PMID: 35990634 Free PMC article.
-
Metformin Enhances the Anti-Cancer Efficacy of Sorafenib via Suppressing MAPK/ERK/Stat3 Axis in Hepatocellular Carcinoma.Int J Mol Sci. 2022 Jul 22;23(15):8083. doi: 10.3390/ijms23158083. Int J Mol Sci. 2022. PMID: 35897659 Free PMC article.
-
Comparing Immunotherapy Versus Chemotherapy Alone as Second-Line Therapy for Malignant Tumors of the Biliary Tract: A Retrospective Study.Clin Med Insights Oncol. 2025 Feb 16;19:11795549251317012. doi: 10.1177/11795549251317012. eCollection 2025. Clin Med Insights Oncol. 2025. PMID: 39963346 Free PMC article.
References
-
- Benson, A.B. 3rd1, et al. HYPERLINK https://www-ncbi-nlm-nih-gov.ezproxy.unibo.it/pubmed/28476736 NCCN Guidelines Insights: Hepatobiliary Cancers, Version 1.2017. J. Natl. Compr. Canc. Netw. 15 563–573 (2017). - PMC - PubMed
-
- European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer: European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J. Hepatol. 56, 908–943 (2012). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
