

Human embryonic stem cell-derived cardiomyocytes restore function in infarcted hearts of non-human primates
- PMID: 29969440
- PMCID: PMC6329375
- DOI: 10.1038/nbt.4162
Human embryonic stem cell-derived cardiomyocytes restore function in infarcted hearts of non-human primates
Erratum in
-
Erratum: Human embryonic stem cell-derived cardiomyocytes restore function in infarcted hearts of non-human primates.Nat Biotechnol. 2018 Sep 6;36(9):899. doi: 10.1038/nbt0918-899a. Nat Biotechnol. 2018. PMID: 30188532 No abstract available.
Abstract
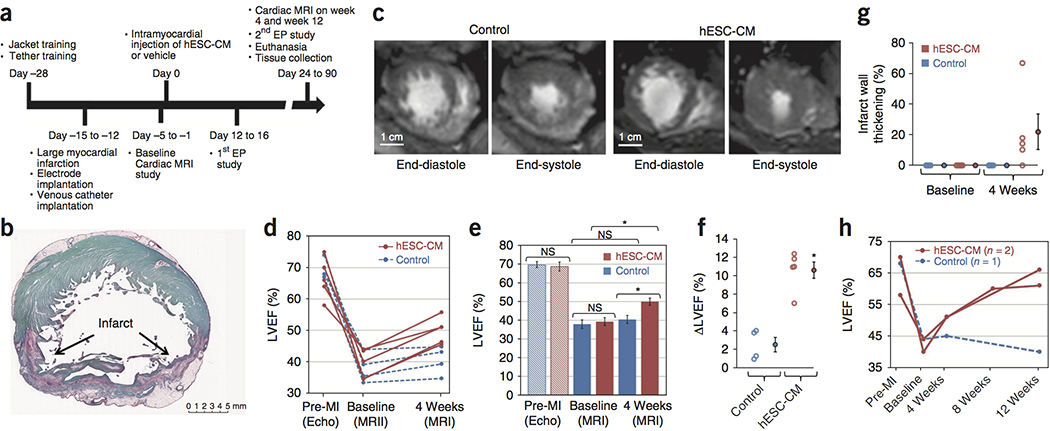
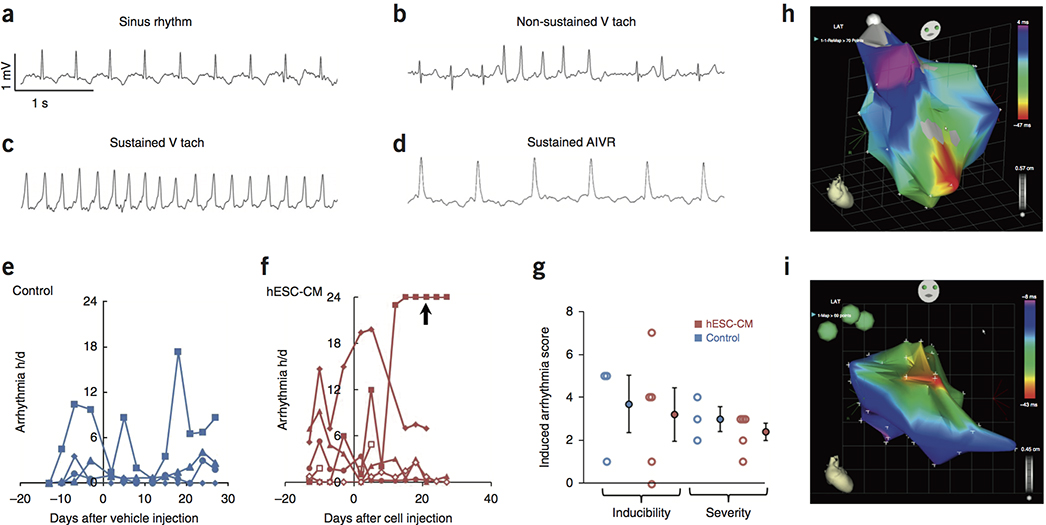
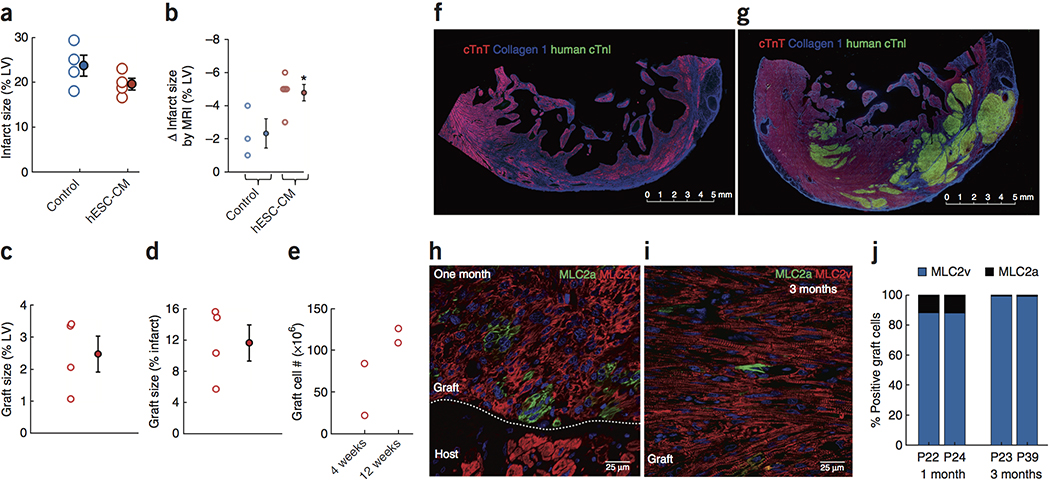
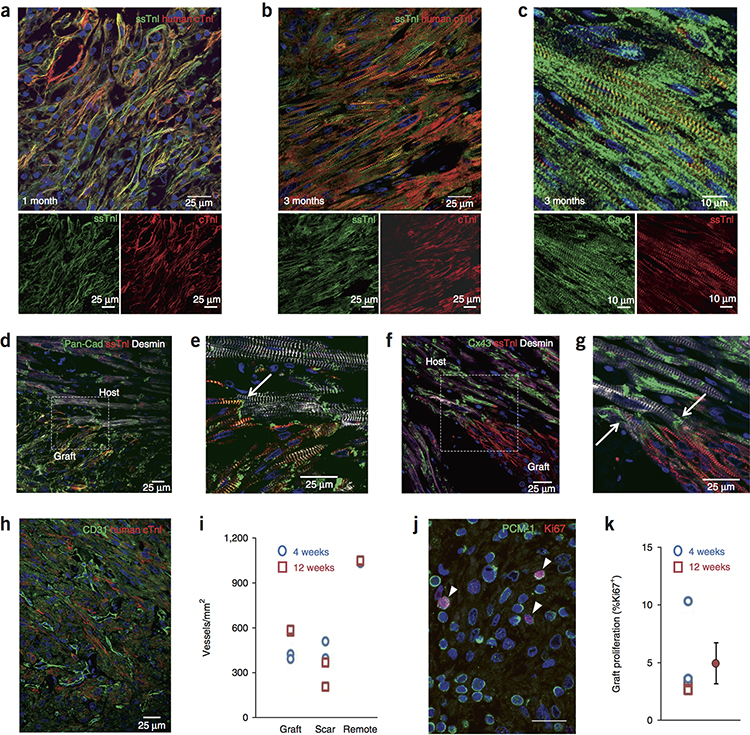
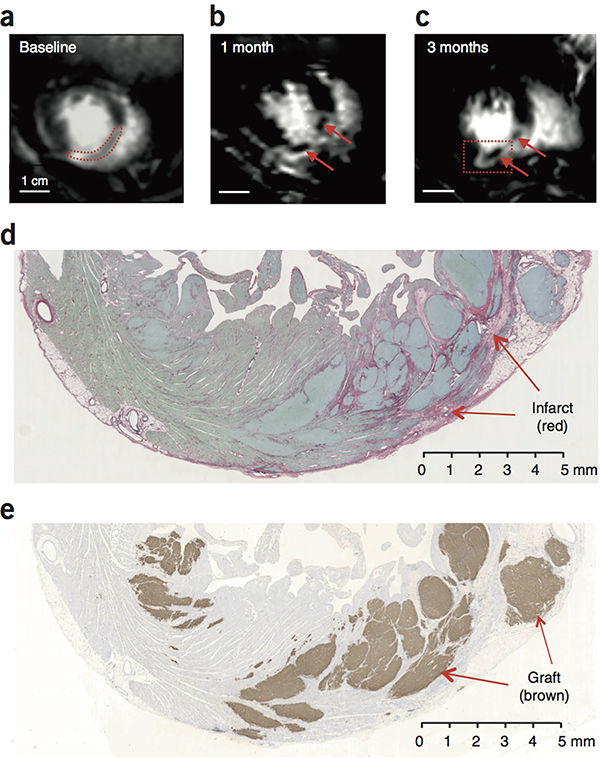
Pluripotent stem cell-derived cardiomyocyte grafts can remuscularize substantial amounts of infarcted myocardium and beat in synchrony with the heart, but in some settings cause ventricular arrhythmias. It is unknown whether human cardiomyocytes can restore cardiac function in a physiologically relevant large animal model. Here we show that transplantation of ∼750 million cryopreserved human embryonic stem cell-derived cardiomyocytes (hESC-CMs) enhances cardiac function in macaque monkeys with large myocardial infarctions. One month after hESC-CM transplantation, global left ventricular ejection fraction improved 10.6 ± 0.9% vs. 2.5 ± 0.8% in controls, and by 3 months there was an additional 12.4% improvement in treated vs. a 3.5% decline in controls. Grafts averaged 11.6% of infarct size, formed electromechanical junctions with the host heart, and by 3 months contained ∼99% ventricular myocytes. A subset of animals experienced graft-associated ventricular arrhythmias, shown by electrical mapping to originate from a point-source acting as an ectopic pacemaker. Our data demonstrate that remuscularization of the infarcted macaque heart with human myocardium provides durable improvement in left ventricular function.
Conflict of interest statement
Drs. Murry, Thies and MacLellan are scientific founders and equity holders in Cytocardia.
Figures
Comment in
-
Stem-cell therapy restores heart function after MI in macaques.Nat Rev Cardiol. 2018 Oct;15(10):582. doi: 10.1038/s41569-018-0062-4. Nat Rev Cardiol. 2018. PMID: 30018375 No abstract available.
-
Moving iPSC-Derived Cardiomyocytes Forward to Treat Myocardial Infarction.Cell Stem Cell. 2018 Sep 6;23(3):322-323. doi: 10.1016/j.stem.2018.08.011. Cell Stem Cell. 2018. PMID: 30193131
-
Prediction of therapeutic effects of human cardiomyocytes in myocardial infarction using non-human primates model.Ann Transl Med. 2018 Nov;6(Suppl 1):S64. doi: 10.21037/atm.2018.10.33. Ann Transl Med. 2018. PMID: 30613639 Free PMC article. No abstract available.
-
Human Embryonic Stem Cell-Derived Cardiomyocytes.Circ Res. 2019 Apr 12;124(8):1157-1159. doi: 10.1161/CIRCRESAHA.119.314869. Circ Res. 2019. PMID: 30973816 No abstract available.
References
-
- Soonpaa MH, Field LJ. Survey of studies examining mammalian cardiomyocyte DNA synthesis. Circ Res. 1998;83:15–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
