

Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies
- PMID: 29969463
- PMCID: PMC6029765
- DOI: 10.1371/journal.pmed.1002595
Adherence interventions and outcomes of tuberculosis treatment: A systematic review and meta-analysis of trials and observational studies
Abstract
Background: Incomplete adherence to tuberculosis (TB) treatment increases the risk of delayed culture conversion with continued transmission in the community, as well as treatment failure, relapse, and development or amplification of drug resistance. We conducted a systematic review and meta-analysis of adherence interventions, including directly observed therapy (DOT), to determine which approaches lead to improved TB treatment outcomes.
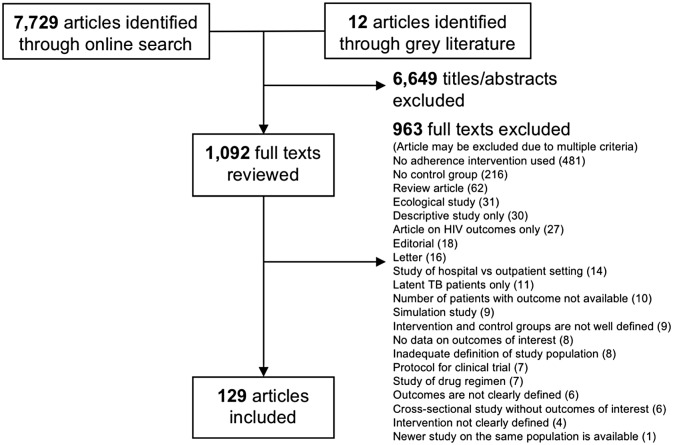
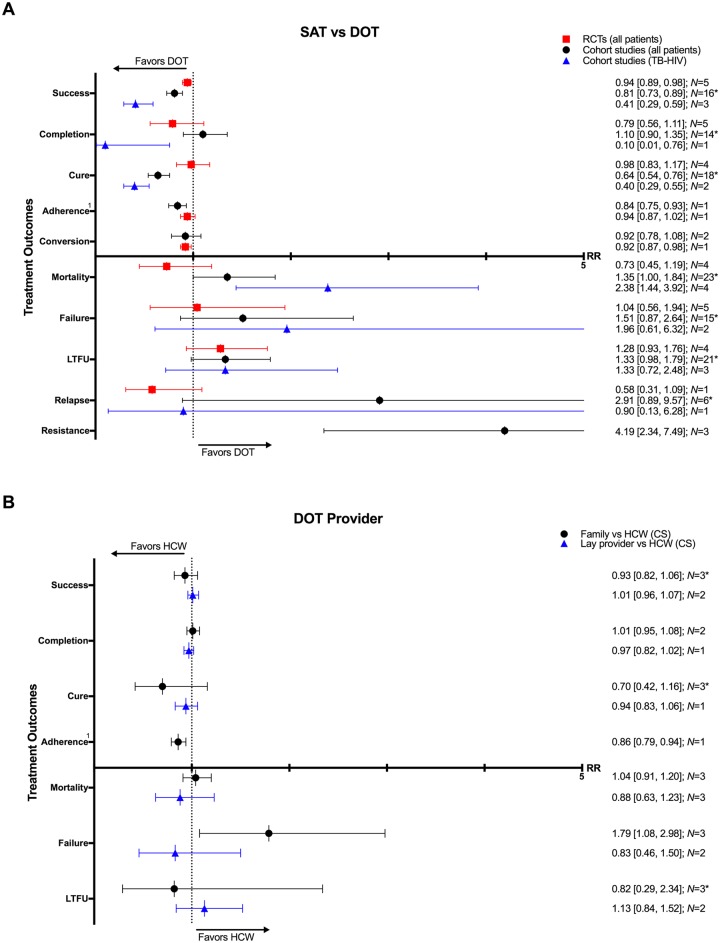
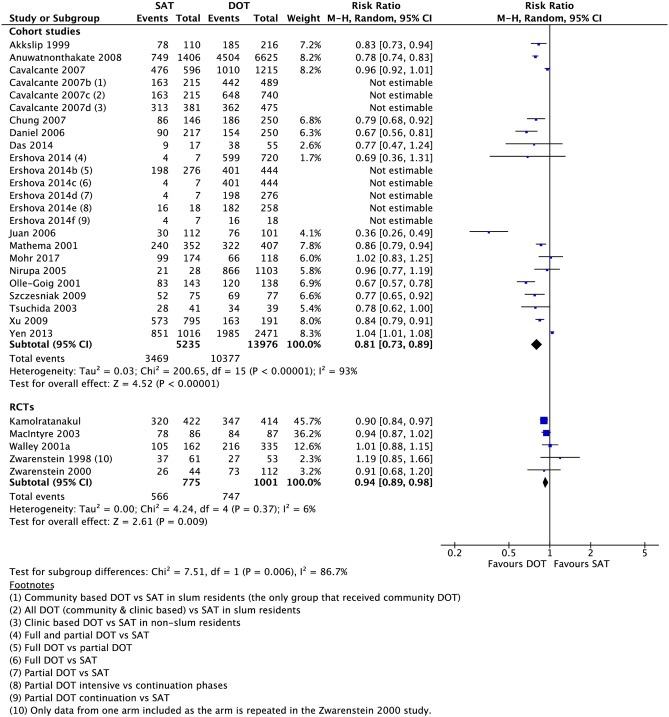
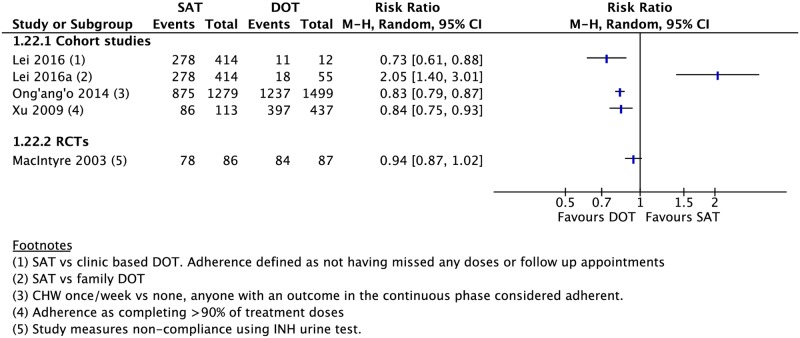
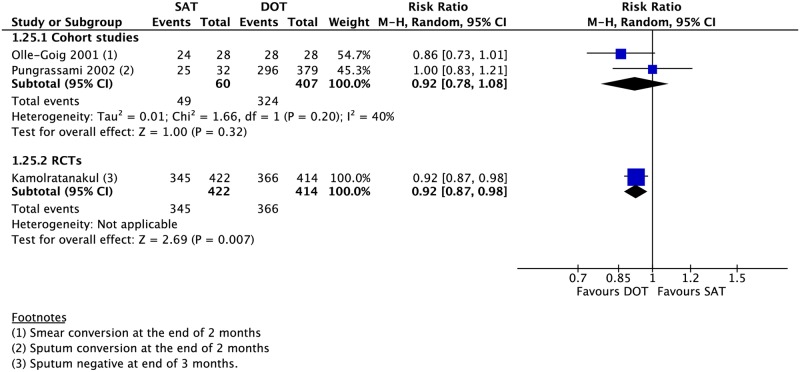
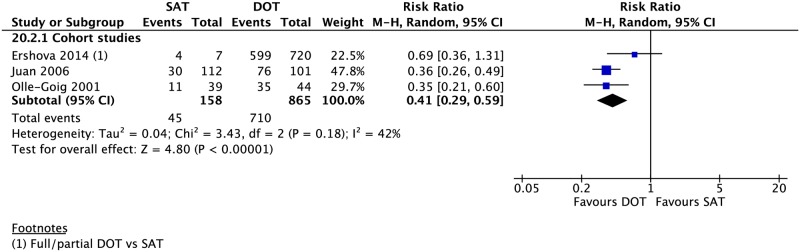
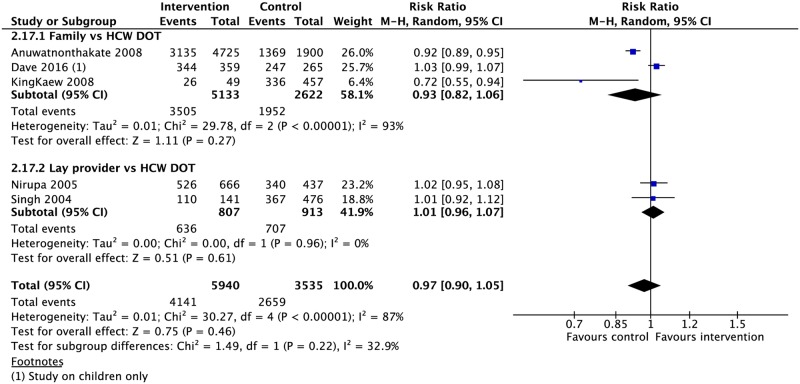
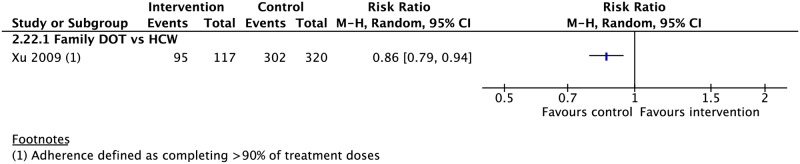
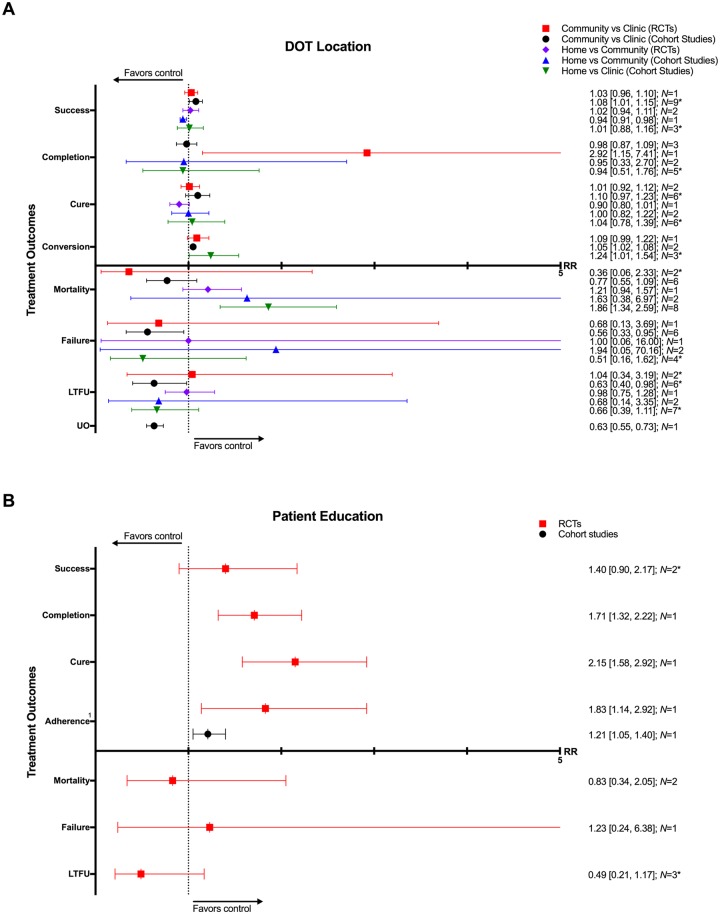
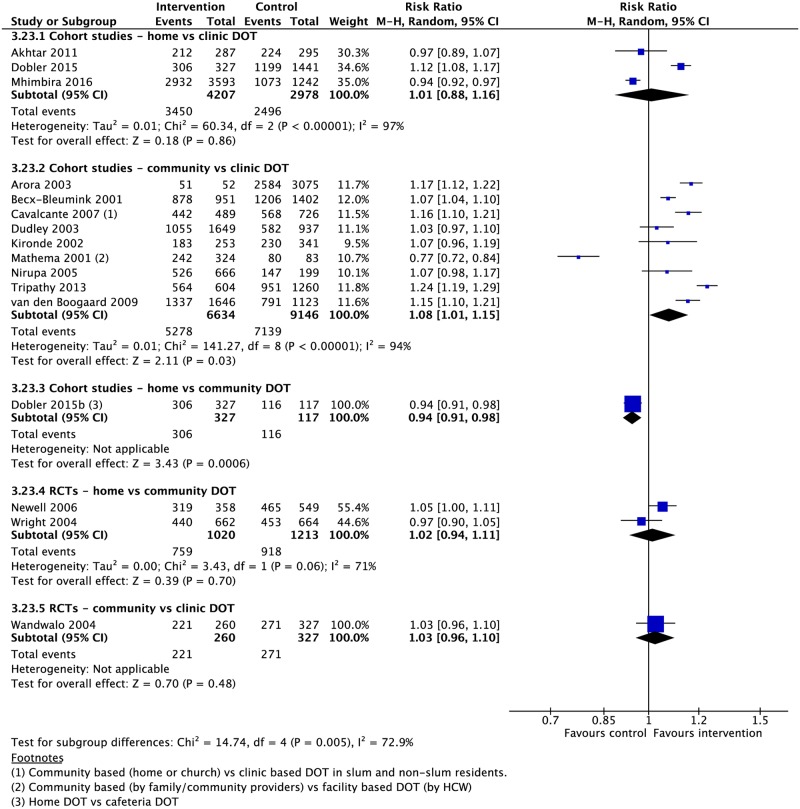
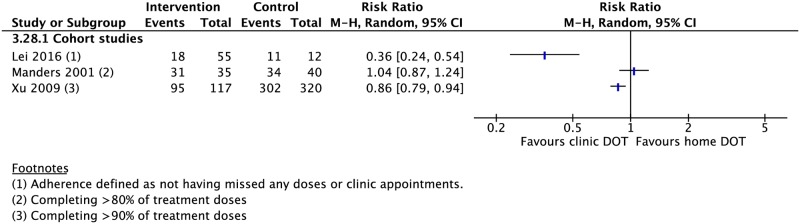
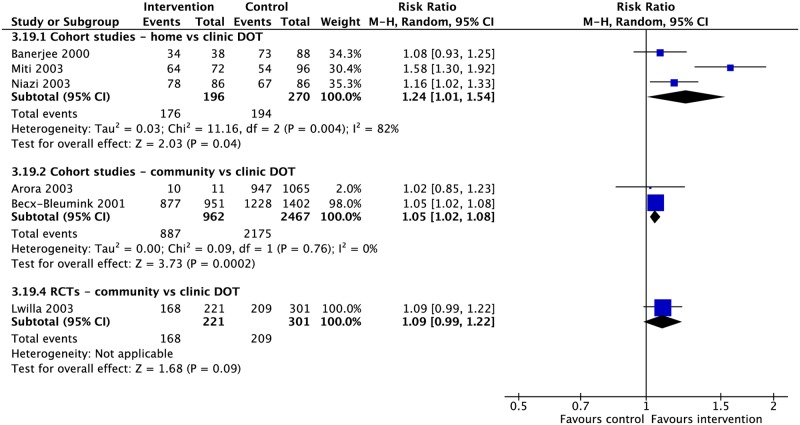
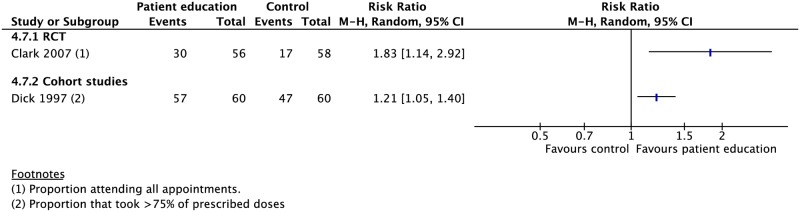
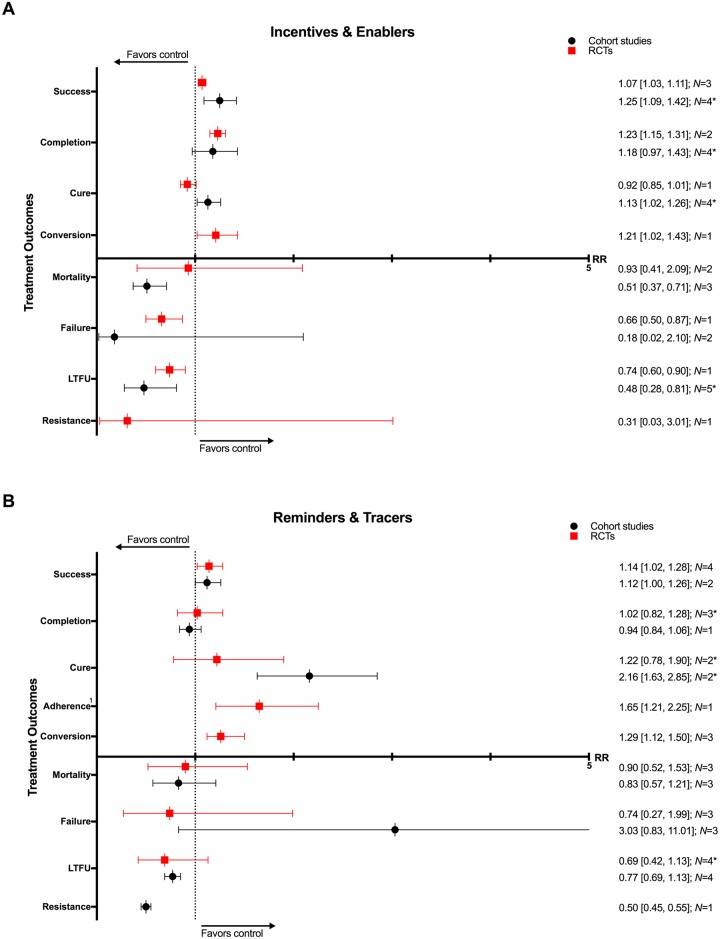
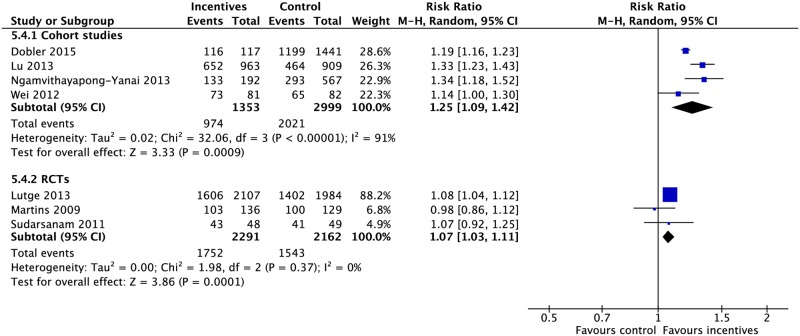
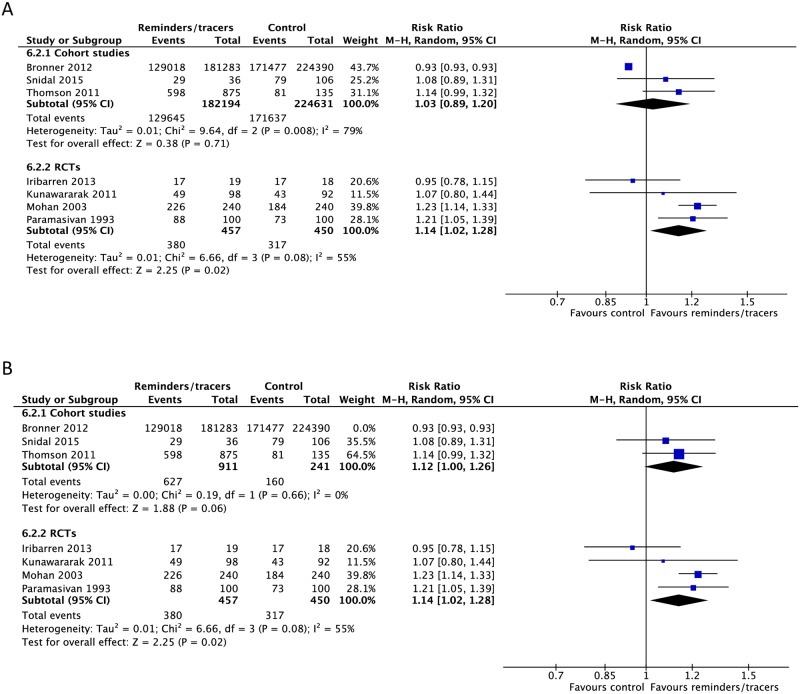
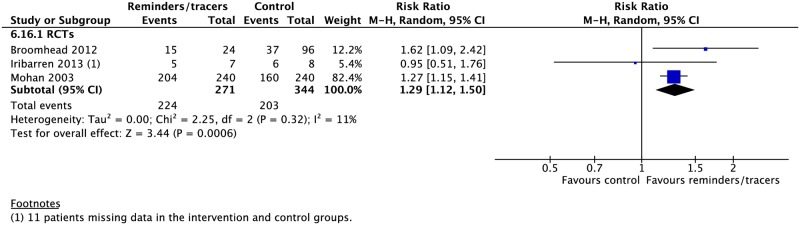
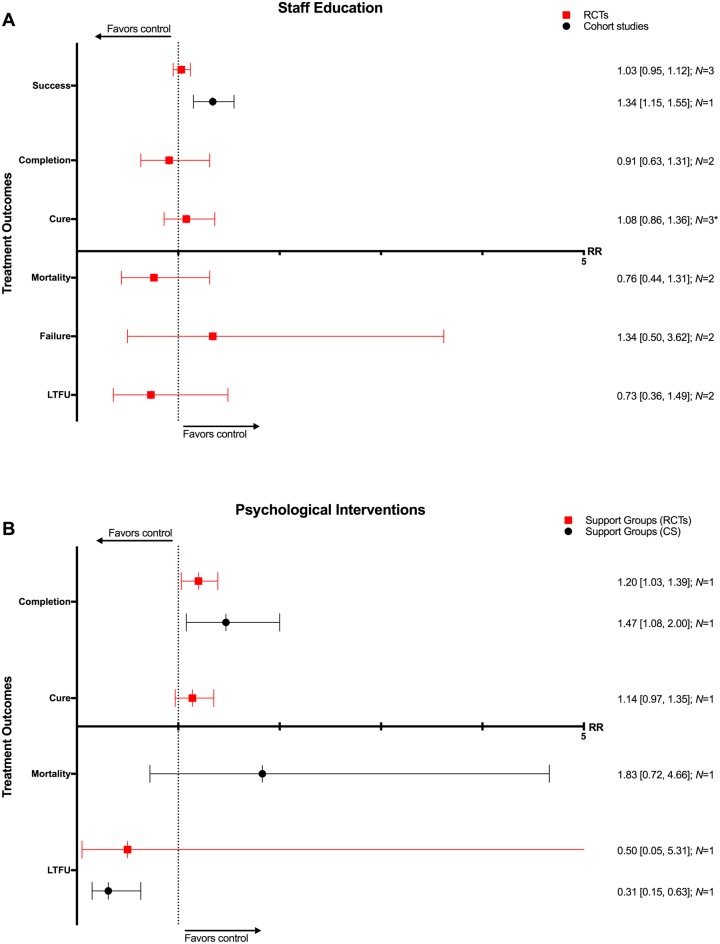
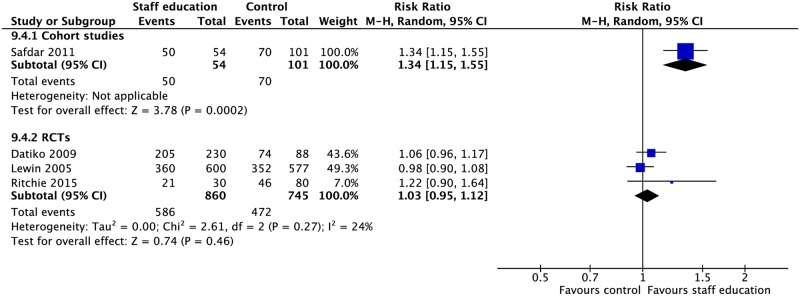
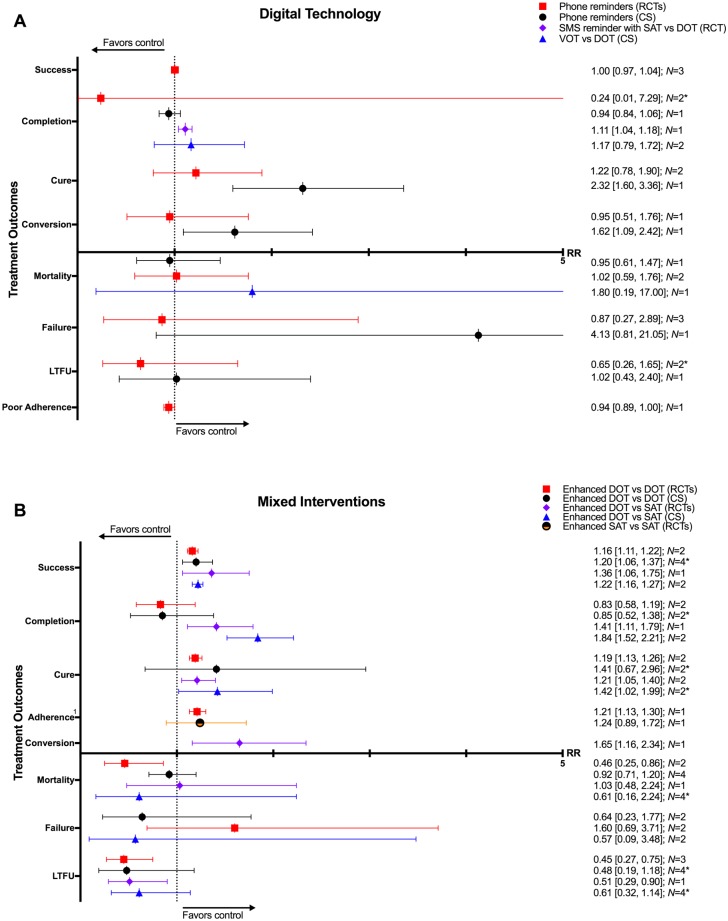
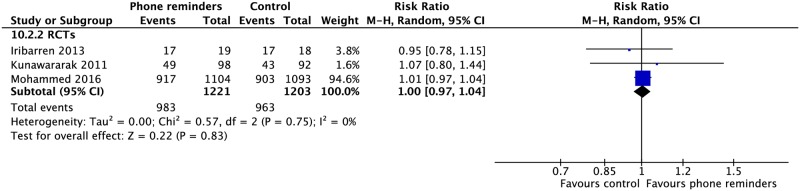
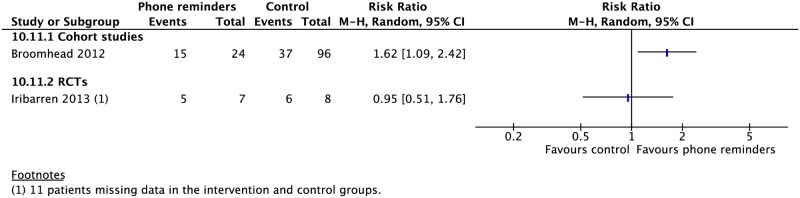
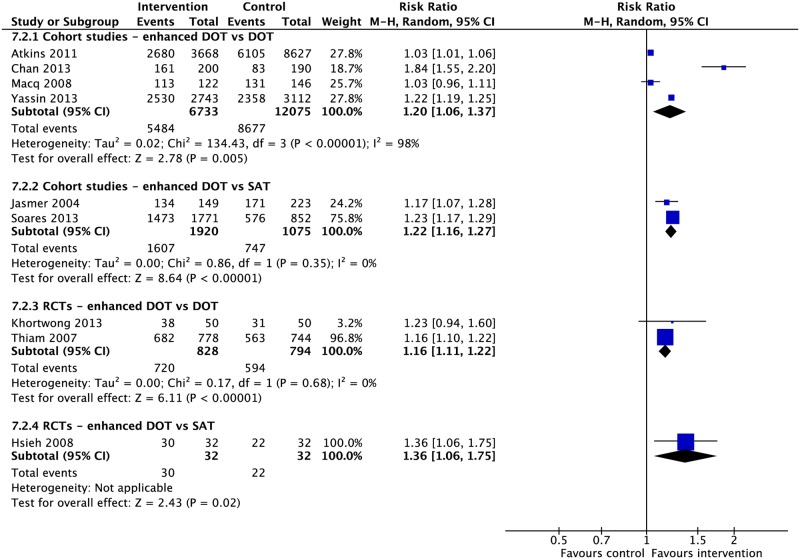
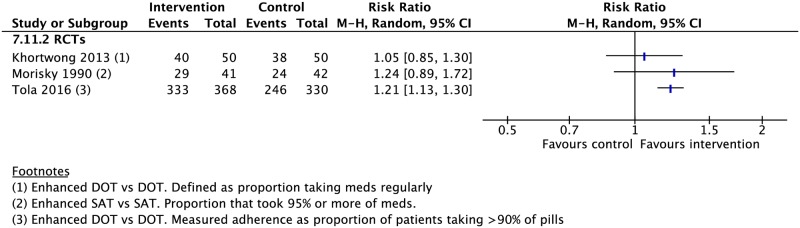
Methods and findings: We systematically reviewed Medline as well as the references of published review articles for relevant studies of adherence to multidrug treatment of both drug-susceptible and drug-resistant TB through February 3, 2018. We included randomized controlled trials (RCTs) as well as prospective and retrospective cohort studies (CSs) with an internal or external control group that evaluated any adherence intervention and conducted a meta-analysis of their impact on TB treatment outcomes. Our search identified 7,729 articles, of which 129 met the inclusion criteria for quantitative analysis. Seven adherence categories were identified, including DOT offered by different providers and at various locations, reminders and tracers, incentives and enablers, patient education, digital technologies (short message services [SMSs] via mobile phones and video-observed therapy [VOT]), staff education, and combinations of these interventions. When compared with DOT alone, self-administered therapy (SAT) was associated with lower rates of treatment success (CS: risk ratio [RR] 0.81, 95% CI 0.73-0.89; RCT: RR 0.94, 95% CI 0.89-0.98), adherence (CS: RR 0.83, 95% CI 0.75-0.93), and sputum smear conversion (RCT: RR 0.92, 95% CI 0.87-0.98) as well as higher rates of development of drug resistance (CS: RR 4.19, 95% CI 2.34-7.49). When compared to DOT provided by healthcare providers, DOT provided by family members was associated with a lower rate of adherence (CS: RR 0.86, 95% CI 0.79-0.94). DOT delivery in the community versus at the clinic was associated with a higher rate of treatment success (CS: RR 1.08, 95% CI 1.01-1.15) and sputum conversion at the end of two months (CS: RR 1.05, 95% CI 1.02-1.08) as well as lower rates of treatment failure (CS: RR 0.56, 95% CI 0.33-0.95) and loss to follow-up (CS: RR 0.63, 95% CI 0.40-0.98). Medication monitors improved adherence and treatment success and VOT was comparable with DOT. SMS reminders led to a higher treatment completion rate in one RCT and were associated with higher rates of cure and sputum conversion when used in combination with medication monitors. TB treatment outcomes improved when patient education, healthcare provider education, incentives and enablers, psychological interventions, reminders and tracers, or mobile digital technologies were employed. Our findings are limited by the heterogeneity of the included studies and lack of standardized research methodology on adherence interventions.
Conclusion: TB treatment outcomes are improved with the use of adherence interventions, such as patient education and counseling, incentives and enablers, psychological interventions, reminders and tracers, and digital health technologies. Trained healthcare providers as well as community delivery provides patient-centered DOT options that both enhance adherence and improve treatment outcomes as compared to unsupervised, SAT alone.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: DF, EJ, and NNL are staff members of the World Health Organization (WHO).
Figures


References
-
- Hirpa S, Medhin G, Girma B, Melese M, Mekonen A, Suarez P, et al. Determinants of multidrug-resistant tuberculosis in patients who underwent first-line treatment in Addis Ababa: a case control study. BMC Public Health. 2013;13:782 Epub 2013/08/29. doi: 10.1186/1471-2458-13-782 . - DOI - PMC - PubMed
-
- Moonan PK, Quitugua TN, Pogoda JM, Woo G, Drewyer G, Sahbazian B, et al. Does directly observed therapy (DOT) reduce drug resistant tuberculosis? BMC Public Health. 2011;11:19 Epub 2011/01/11. doi: 10.1186/1471-2458-11-19 . - DOI - PMC - PubMed
-
- Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238 doi: 10.1371/journal.pmed.0040238 . - DOI - PMC - PubMed
-
- Weis SE, Slocum PC, Blais FX, King B, Nunn M, Matney GB, et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N Engl J Med. 1994;330(17):1179–84. Epub 1994/04/28. doi: 10.1056/NEJM199404283301702 . - DOI - PubMed
-
- Ormerod LP, Prescott RJ. Inter-relations between relapses, drug regimens and compliance with treatment in tuberculosis. Respir Med. 1991;85(3):239–42. Epub 1991/05/01. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
