

Expanding laparoscopic pancreaticoduodenectomy to pancreatic-head and periampullary malignancy: major findings based on systematic review and meta-analysis
- PMID: 29969999
- PMCID: PMC6029373
- DOI: 10.1186/s12876-018-0830-y
Expanding laparoscopic pancreaticoduodenectomy to pancreatic-head and periampullary malignancy: major findings based on systematic review and meta-analysis
Abstract
Background: Laparoscopic pancreaticoduodenectomy (LPD) remains to be established as a safe and effective alternative to open pancreaticoduodenectomy (OPD) for pancreatic-head and periampullary malignancy. The purpose of this meta-analysis was to compare LPD with OPD for these malignancies regarding short-term surgical and long-term survival outcomes.
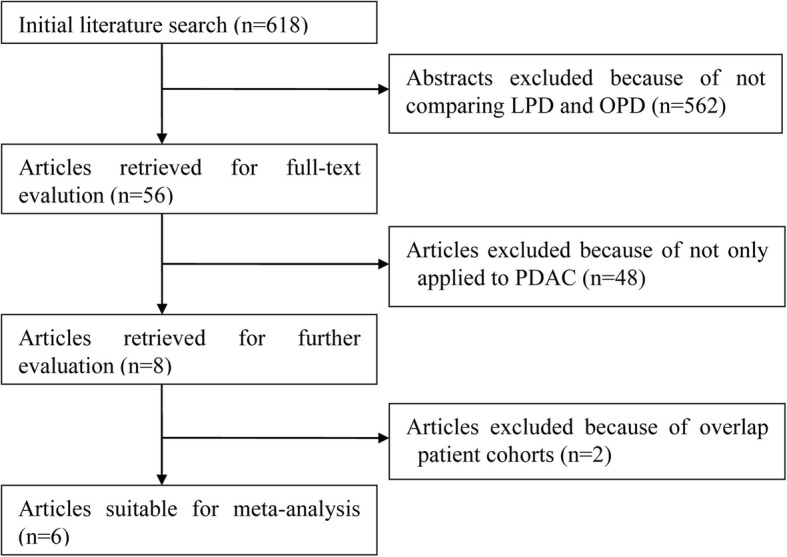
Methods: A literature search was conducted before March 2018 to identify comparative studies in regard to outcomes of both LPD and OPD for the treatment of pancreatic-head and periampullary malignancies. Morbidity, postoperative pancreatic fistula (POPF), mortality, operative time, estimated blood loss, hospitalization, retrieved lymph nodes, and survival outcomes were compared.
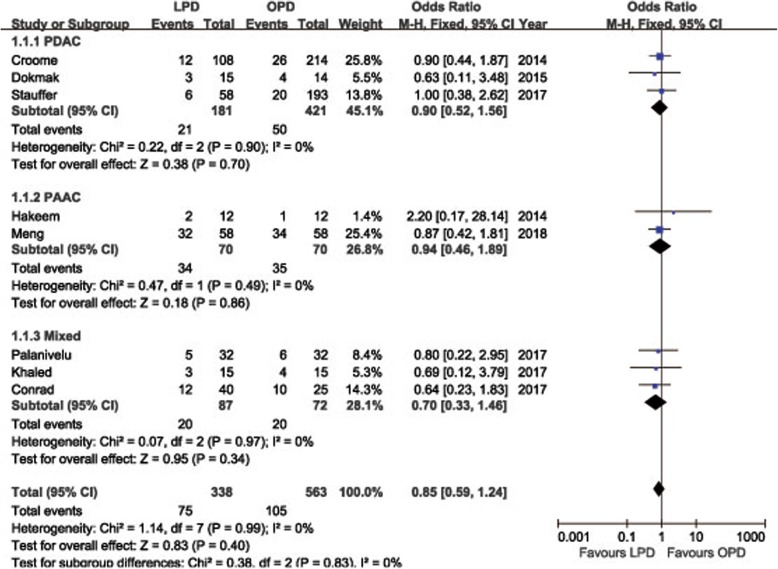
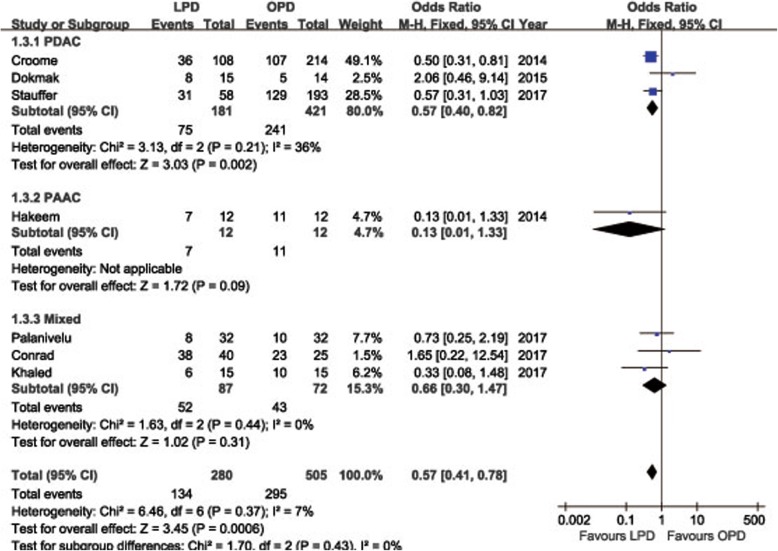
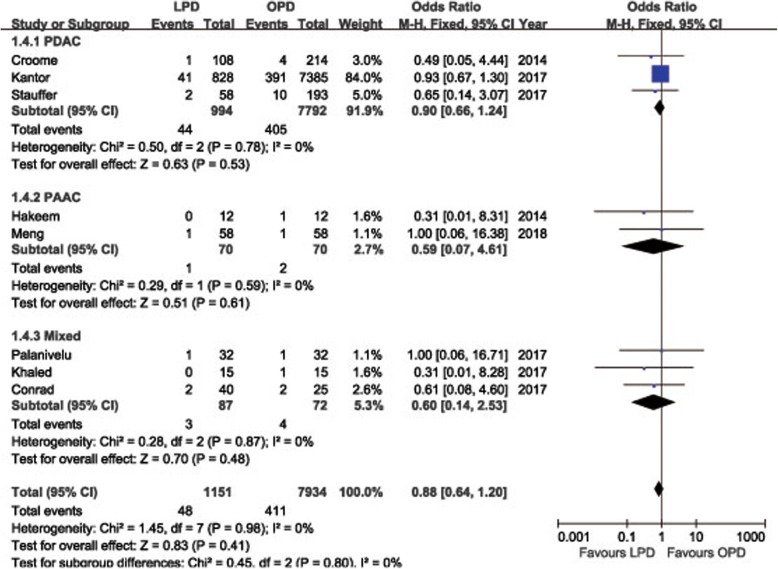
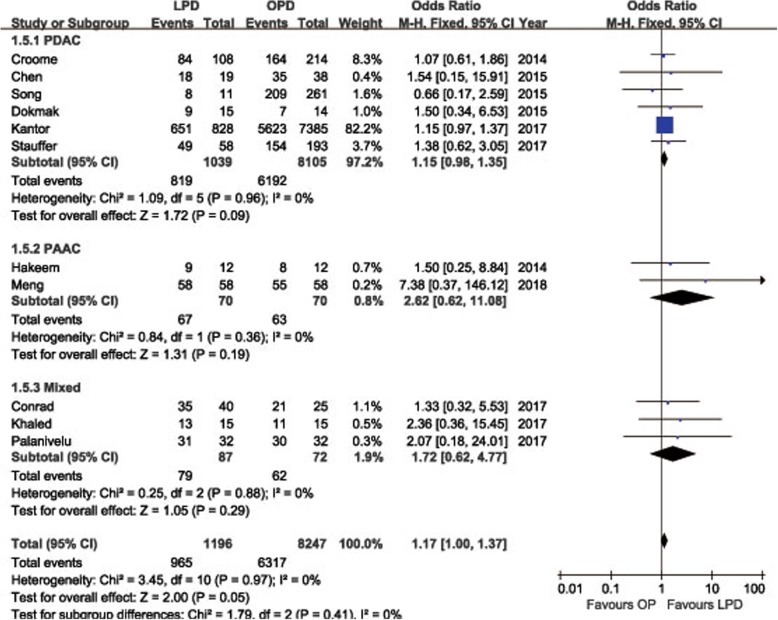
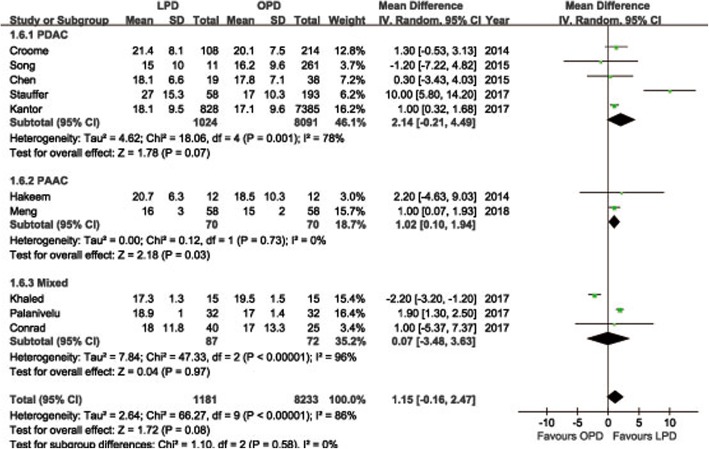
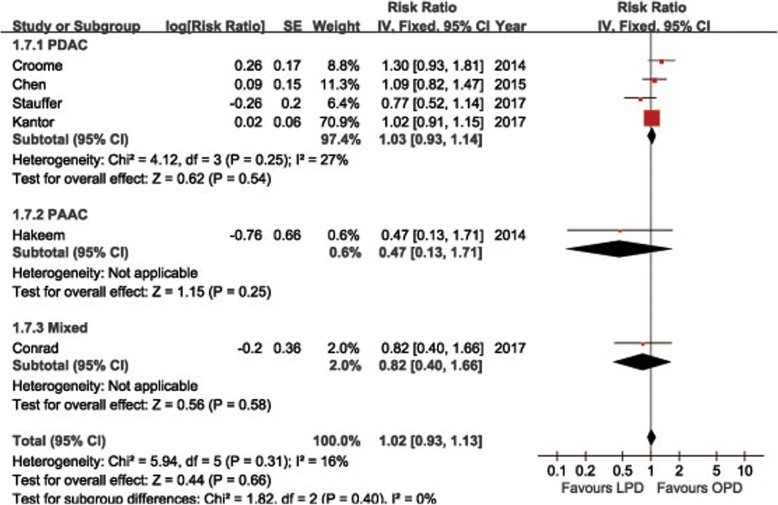
Results: Among eleven identified studies, 1196 underwent LPD, and 8247 were operated through OPD. The pooled data showed that LPD was associated with less morbidity (OR = 0.57, 95%CI: 0.41~ 0.78, P < 0.01), less blood loss (WMD = - 372.96 ml, 95% CI, - 507.83~ - 238.09 ml, P < 0.01), shorter hospital stays (WMD = - 197.49 ml, 95% CI, - 304.62~ - 90.37 ml, P < 0.01), and comparable POPF (OR = 0.85, 95%CI: 0.59~ 1.24, P = 0.40), and overall survival (HR = 1.03, 95%CI: 0.93~ 1.14, P = 0.54) compared to OPD. Operative time was longer in LPD (WMD = 87.68 min; 95%CI: 27.05~ 148.32, P < 0.01), whereas R0 rate tended to be higher in LPD (OR = 1.17; 95%CI: 1.00~ 1.37, P = 0.05) and there tended to be more retrieved lymph nodes in LPD (WMD = 1.15, 95%CI: -0.16~ 2.47, P = 0.08), but these differences failed to reach statistical significance.
Conclusions: LPD can be performed as safe and effective as OPD for pancreatic-head and periampullary malignancy with respect to both surgical and oncological outcomes. LPD is associated with less intraoperative blood loss and postoperative morbidity and may serve as a promising alternative to OPD in selected individuals in the future.
Keywords: Adenocarcinoma; Laparoscopy; Meta-analysis; Morbidity; Pancreaticoduodenectomy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Neoptolemos JP, Moore MJ, Cox TF, Valle JW, Palmer DH, McDonald AC, Carter R, Tebbutt NC, Dervenis C, Smith D, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: the ESPAC-3 periampullary cancer randomized trial. Jama. 2012;308(2):147–156. doi: 10.1001/jama.2012.7352. - DOI - PubMed
-
- Ricci C, Casadei R, Taffurelli G, Toscano F, Pacilio CA, Bogoni S, D'Ambra M, Pagano N, Di Marco MC, Minni F. Laparoscopic versus open distal pancreatectomy for ductal adenocarcinoma: a systematic review and meta-analysis. J Gastrointest Surg. 2015;19(4):770–781. doi: 10.1007/s11605-014-2721-z. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
