

Proton versus photon deep inspiration breath hold technique in patients with hodgkin lymphoma and mediastinal radiation : A PLANNING COMPARISON OF DEEP INSPIRATION BREATH HOLD INTENSITY MODULATION RADIOTHERAPY AND INTENSITY MODULATED PROTON THERAPY
- PMID: 29970105
- PMCID: PMC6029162
- DOI: 10.1186/s13014-018-1066-2
Proton versus photon deep inspiration breath hold technique in patients with hodgkin lymphoma and mediastinal radiation : A PLANNING COMPARISON OF DEEP INSPIRATION BREATH HOLD INTENSITY MODULATION RADIOTHERAPY AND INTENSITY MODULATED PROTON THERAPY
Abstract
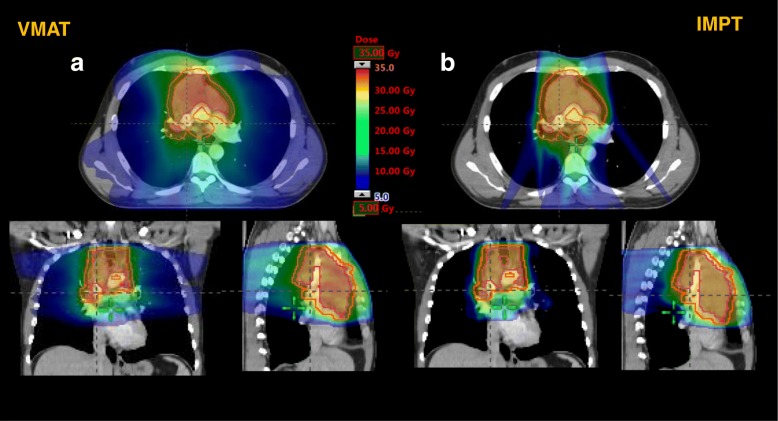
Background: The benefits of proton therapy in the treatment of patients with Hodgkin lymphoma (HL) are controversially discussed. Therefore we compared intensitiy modulated proton therapy (IMPT) with intensity modulated radiotherapy (IMRT), in the form of volumetric modulated arc therapy (VMAT) in patients with Hodgkin lymphoma (HL), through a comparative treatment planning study.
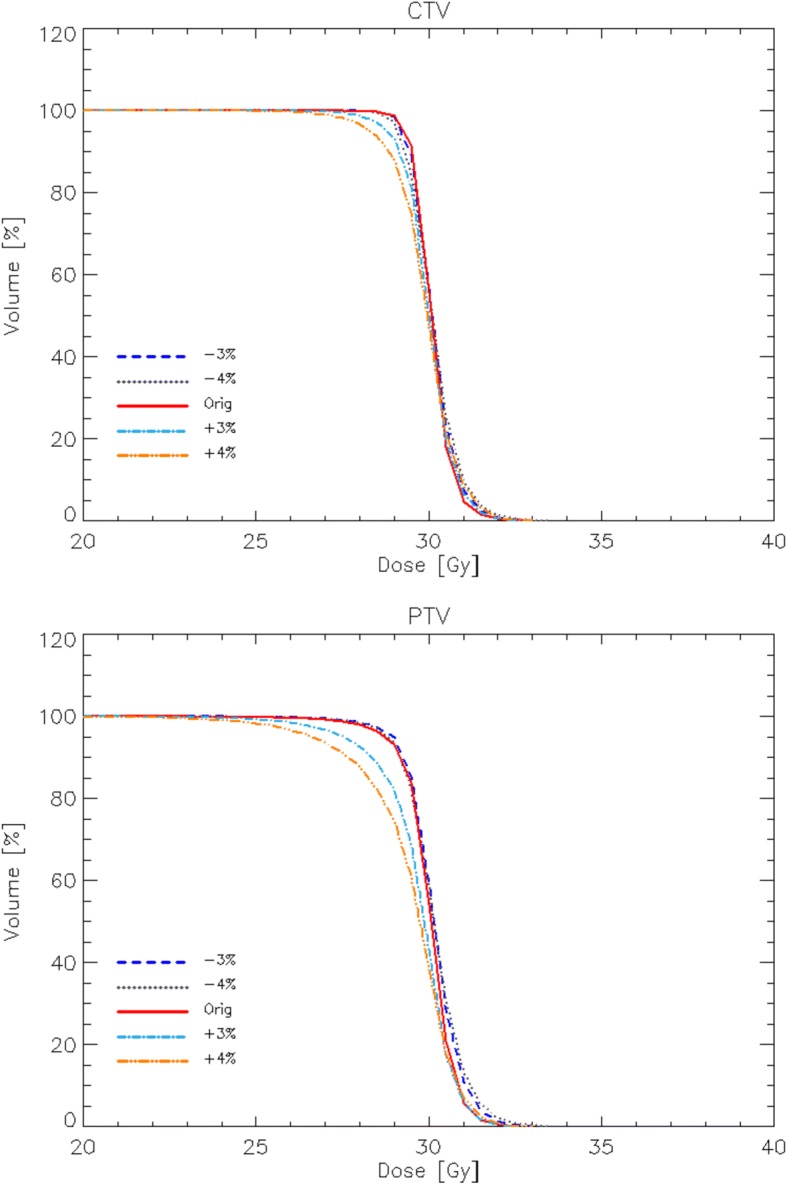
Methods: Radiation plans for 21 patients with Hodgkin Lymphoma (HL) were computed for IMPT and deep inspiration breath hold (DIBH) VMAT. Plans were optimized and computed assuming deep inspiration breath holding conditions. Dosimetric comparison on standard metrics from dose volume histograms was performed to appraise the relative merits of the two techniques, while proton plan robustness was assessed by re-computing the dose distribution of each plan by varying the Hounsfield Units to stopping power calibration by applying a ± 3 and 4% error.
Results: DIBH-VMAT and IMPT both provided excellent coverage, conformity and heterogeneity of the clinical target volume (CTV) and planning target volume (PTV). IMPT reduced mean doses to the breasts, lungs, heart and normal tissue by 38-83%. IMPT significantly reduced mean doses to the heart to < 5 Gy despite bulky mediastinal disease and decreased breast doses in female patients to < 1 Gy. Despite the simulated 3 and 4% miscalibration errors, no remarkable or measurable impact was observed on the organs at risk (OARs).
Conclusions: This is the first comparison between DIBH-VMAT and IMPT in HL treatment. We could demonstrate statistically significant decreases in all dose/volume metrics of the OARs. Regardless of the planning paradigm used, range uncertainties can substantially under dose the PTV, while perhaps not leading to clinically significant deterioration of CTV coverage. With the geometry applied no impact was observed for OARs, suggesting IMPT as a superior technique for potentially reducing future health risks for HL patients.
Keywords: Hodgkin lymphoma; Proton beam therapy; Range uncertainties; VMAT.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Dr. L. Cozzi acts as Scientific Advisor to Varian Medical Systems. Other authors have no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Maraldo MV, Brodin NP, Aznar MC, Vogelius IR, Munck af Rosenschöld P, Petersen PM, et al. Estimated risk of cardiovascular disease and secondary cancers with modern highly conformal radiotherapy for early-stage mediastinal Hodgkin lymphoma. Ann Oncol. 2013;24:2113–2118. doi: 10.1093/annonc/mdt156. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
