

Inhibition of CRTH2-mediated Th2 activation attenuates pulmonary hypertension in mice
- PMID: 29970474
- PMCID: PMC6080901
- DOI: 10.1084/jem.20171767
Inhibition of CRTH2-mediated Th2 activation attenuates pulmonary hypertension in mice
Abstract
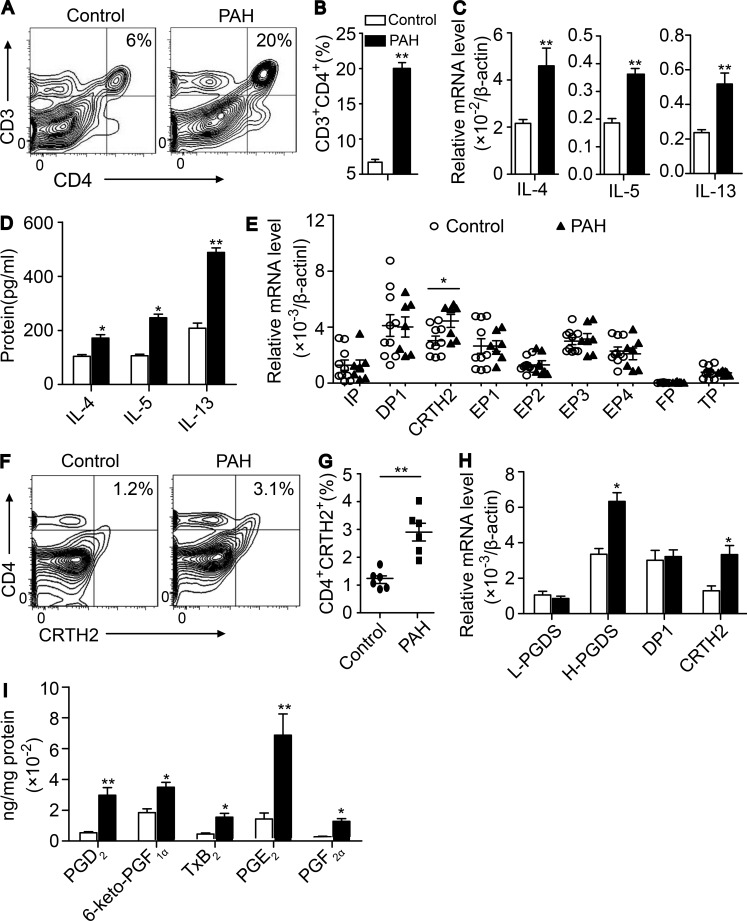
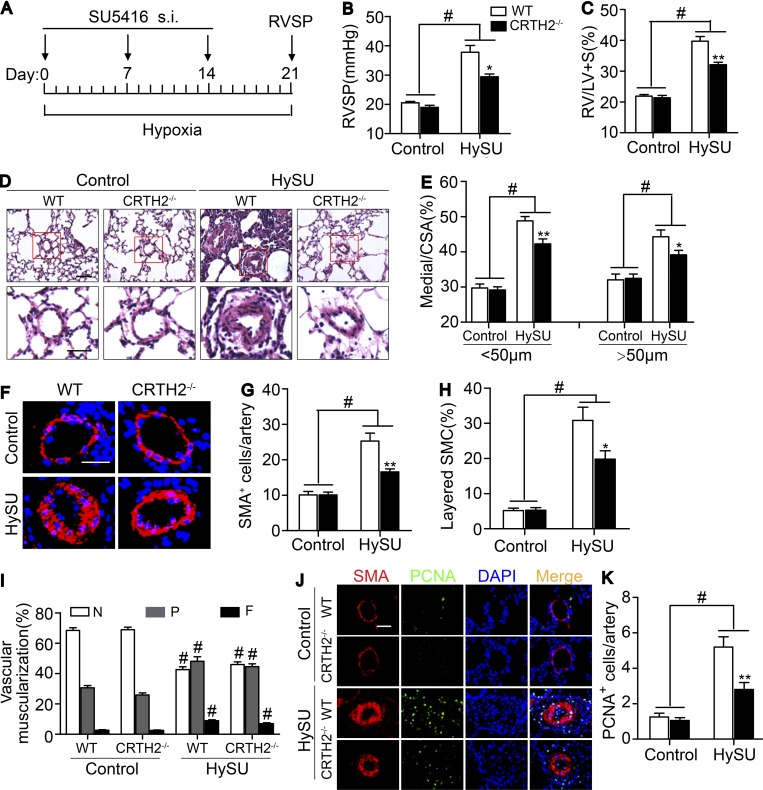
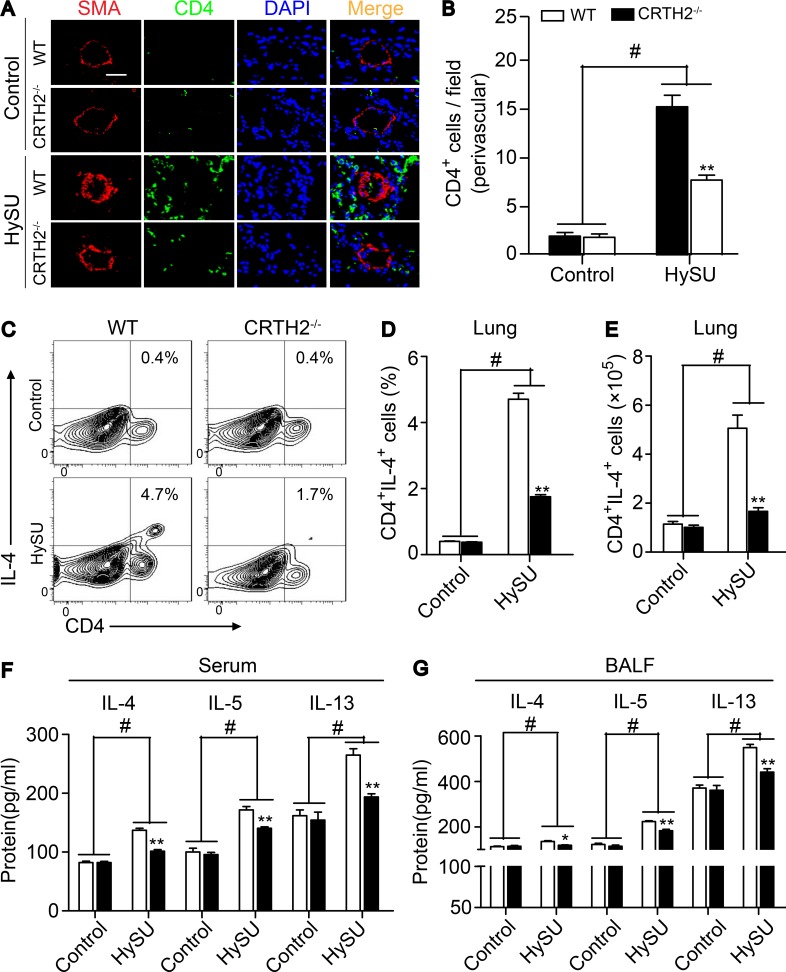
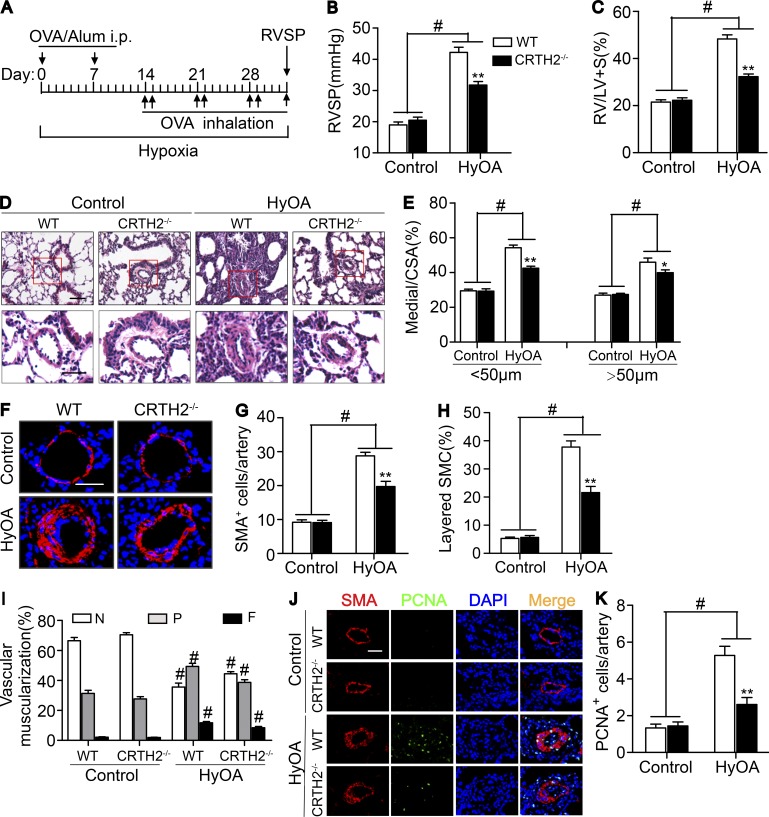
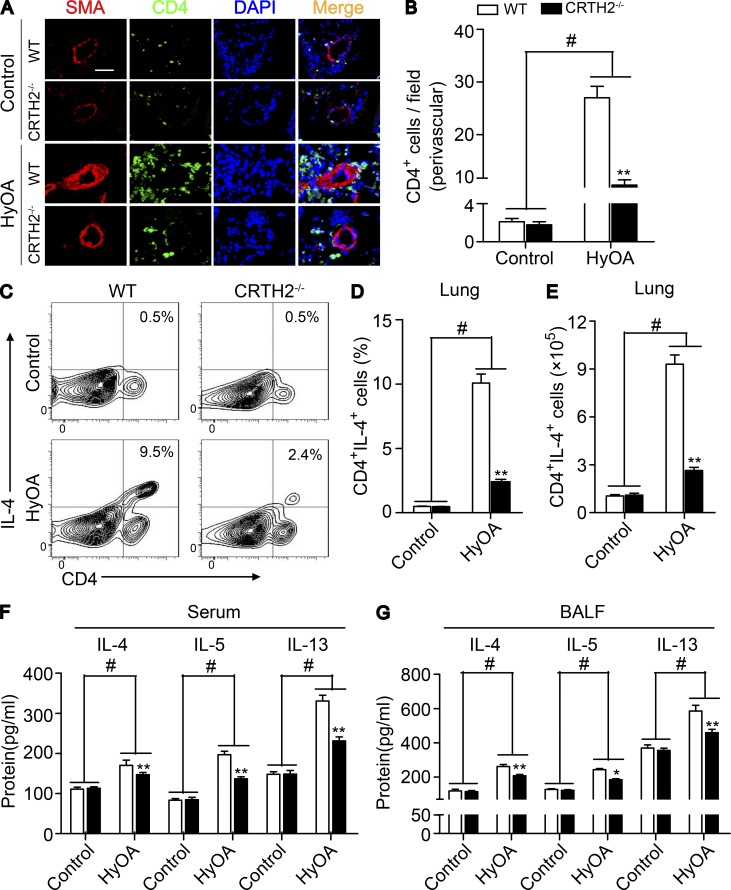
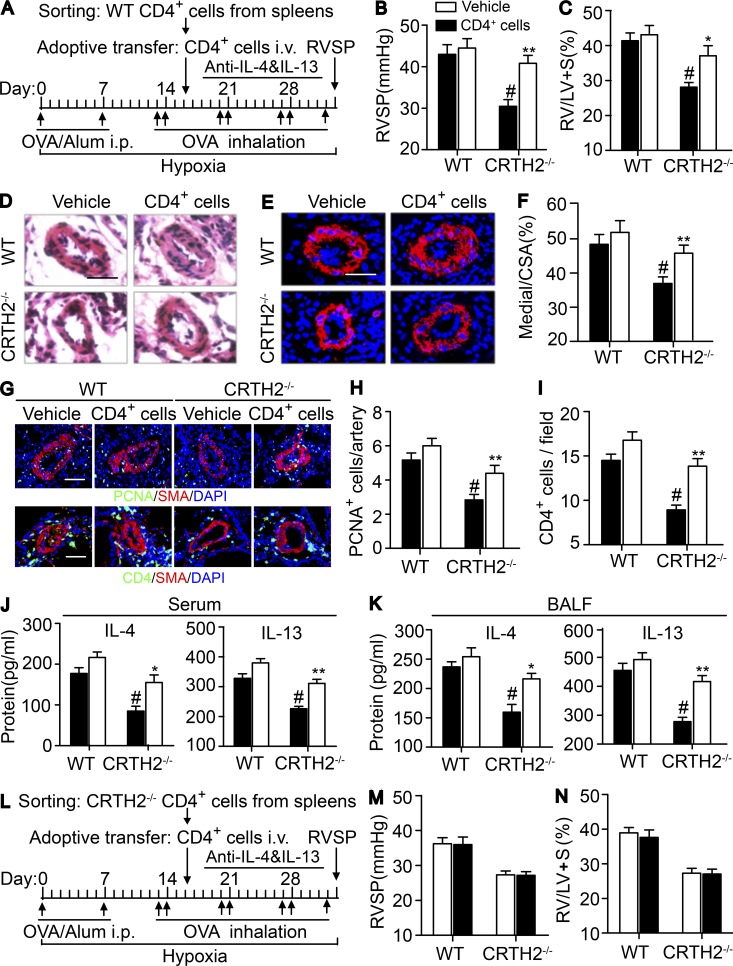
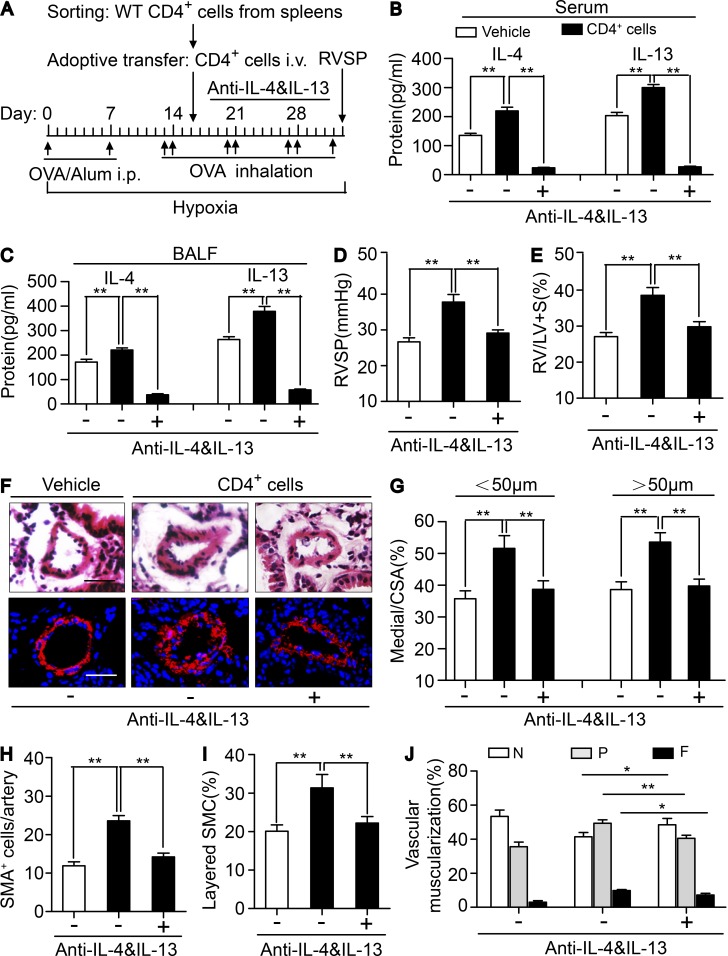
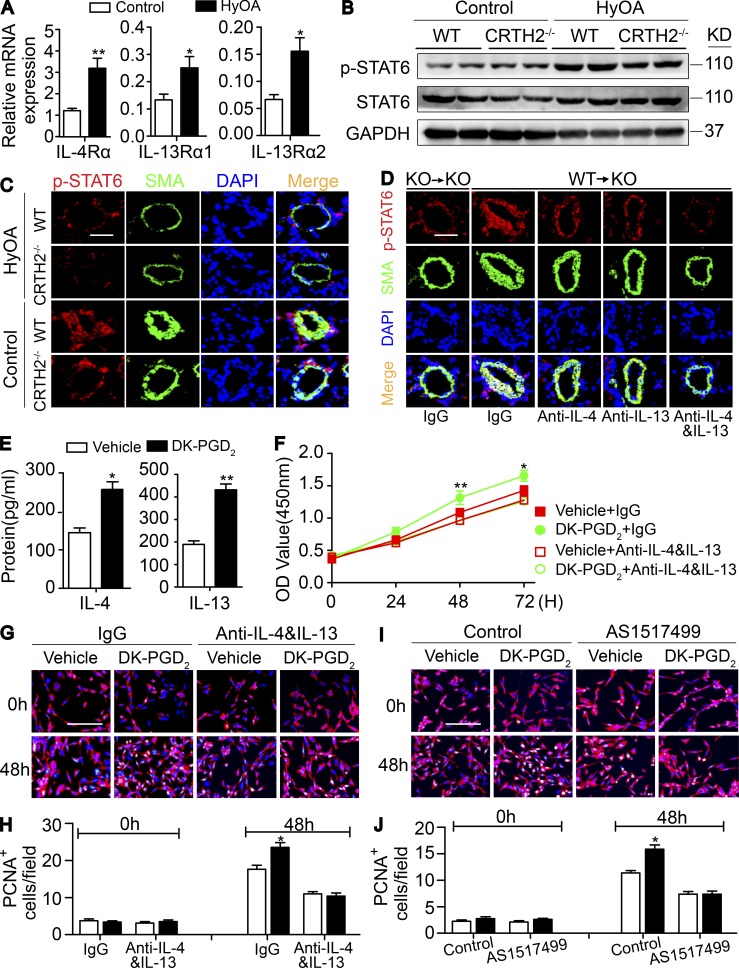
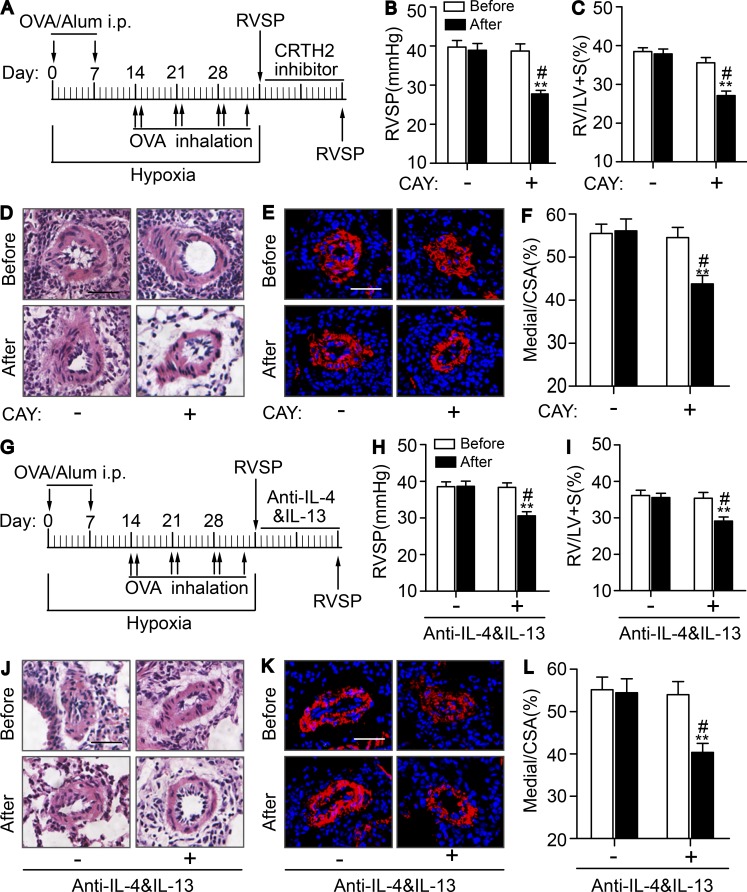
Pulmonary arterial hypertension (PAH) is a life-threatening disease characterized by progressive pulmonary artery (PA) remodeling. T helper 2 cell (Th2) immune response is involved in PA remodeling during PAH progression. Here, we found that CRTH2 (chemoattractant receptor homologous molecule expressed on Th2 cell) expression was up-regulated in circulating CD3+CD4+ T cells in patients with idiopathic PAH and in rodent PAH models. CRTH2 disruption dramatically ameliorated PA remodeling and pulmonary hypertension in different PAH mouse models. CRTH2 deficiency suppressed Th2 activation, including IL-4 and IL-13 secretion. Both CRTH2+/+ bone marrow reconstitution and CRTH2+/+ CD4+ T cell adoptive transfer deteriorated hypoxia + ovalbumin-induced PAH in CRTH2-/- mice, which was reversed by dual neutralization of IL-4 and IL-13. CRTH2 inhibition alleviated established PAH in mice by repressing Th2 activity. In culture, CRTH2 activation in Th2 cells promoted pulmonary arterial smooth muscle cell proliferation through activation of STAT6. These results demonstrate the critical role of CRTH2-mediated Th2 response in PAH pathogenesis and highlight the CRTH2 receptor as a potential therapeutic target for PAH.
© 2018 Tianjin Medical University.
Figures
References
-
- Barnes P.J. 2018. Targeting cytokines to treat asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. <ext-link xmlns:xlink="http://www.w3.org/1999/xlink" ext-link-type="uri" xlink:href="http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed..."><underline>PubMed</underline></ext-link> 10.1038/s41577-018-0006-6 - DOI - PubMed
-
- Benza R.L., Miller D.P., Gomberg-Maitland M., Frantz R.P., Foreman A.J., Coffey C.S., Frost A., Barst R.J., Badesch D.B., Elliott C.G., et al. 2010. Predicting survival in pulmonary arterial hypertension: Insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 122:164–172. 10.1161/CIRCULATIONAHA.109.898122 - DOI - PubMed
-
- Bigna J.J., Nansseu J.R., Um L.N., Noumegni S.R., Simé P.S., Aminde L.N., Koulla-Shiro S., and Noubiap J.J.. 2016. Prevalence and incidence of pulmonary hypertension among HIV-infected people in Africa: A systematic review and meta-analysis. BMJ Open. 6:e011921 10.1136/bmjopen-2016-011921 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
