

The Binomial Parasite-Host Immunity in the Healing Process and in Reactivation of Human Tegumentary Leishmaniasis
- PMID: 29971054
- PMCID: PMC6018218
- DOI: 10.3389/fmicb.2018.01308
The Binomial Parasite-Host Immunity in the Healing Process and in Reactivation of Human Tegumentary Leishmaniasis
Abstract
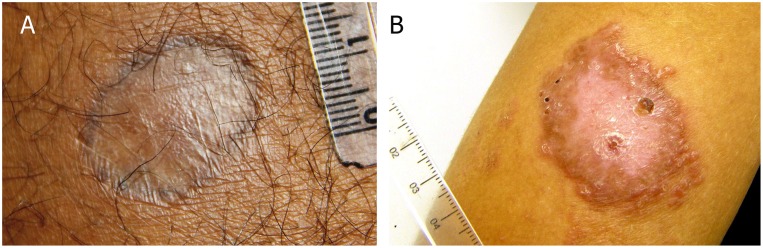
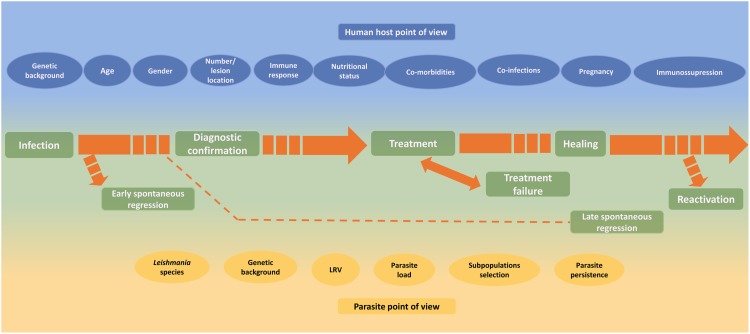
Leishmaniasis is a vector-borne infectious disease caused by different species of protozoa from the Leishmania genus. Classically, the disease can be classified into two main clinical forms: Visceral (VL) and Tegumentary (TL) leishmaniasis. TL is a skin/mucosal granulomatous disease that manifests mainly as cutaneous localized or disseminated ulcers, papules diffusely distributed, mucosal lesions or atypical lesions. Once the etiology of the infection is confirmed, treatment can take place, and different drugs can be administered. It has already been shown that, even when the scar is clinically evident, inflammation is still present in the native tissue, and the decrease of the inflammatory process occurs slowly during the 1st years after clinical healing. The maintenance of residual parasites in the scar tissue is also well documented. Therefore, it is no longer a surprise that, under some circumstances, therapeutic failure and/or lesion reactivation occurs. All over the years, an impressive amount of data on relapses, treatment resistance and lesion reactivation after healing has been collected, and several factors have been pointed out as having a role in the process. Different factors such as Leishmania species, parasite variability, Leishmania RNA virus 1, parasite load, parasite persistence, age, nutritional status, gender, co-morbidities, co-infection, pregnancy, immunosuppression, lesion duration, number and localization of lesions, drug metabolism, irregular treatment and individual host cellular immune response were described and discussed in the present review. Unfortunately, despite this amount of information, a conclusive understanding remains under construction. In addition, multifactorial influence cannot be discarded. In this context, knowing why leishmaniasis has been difficult to treat and control can help the development of new approaches, such as drugs and immunotherapy in order to improve healing maintenance. In this sense, we would like to highlight some of the findings that may influence the course of Leishmania infection and the therapeutic response, with an emphasis on TL.
Keywords: Leishmania parasites; co-morbidities; healing process; immunosuppression; leishmaniasis; lesion reactivation; patients; tegumentary leishmaniasis.
Figures
Similar articles
-
Co-expression analysis of lncRNA and mRNA suggests a role for ncRNA-mediated regulation of host-parasite interactions in primary skin lesions of patients with American tegumentary leishmaniasis.Acta Trop. 2023 Sep;245:106966. doi: 10.1016/j.actatropica.2023.106966. Epub 2023 Jun 9. Acta Trop. 2023. PMID: 37302689
-
Multiparametric analysis of host and parasite elements in new world tegumentary leishmaniasis.Front Cell Infect Microbiol. 2022 Aug 9;12:956112. doi: 10.3389/fcimb.2022.956112. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36017367 Free PMC article.
-
Insulin-like growth factor-I serum levels and their biological effects on Leishmania isolates from different clinical forms of American tegumentary leishmaniasis.Parasit Vectors. 2016 Jun 11;9(1):335. doi: 10.1186/s13071-016-1619-x. Parasit Vectors. 2016. PMID: 27286813 Free PMC article.
-
PKDL and other dermal lesions in HIV co-infected patients with Leishmaniasis: review of clinical presentation in relation to immune responses.PLoS Negl Trop Dis. 2014 Nov 20;8(11):e3258. doi: 10.1371/journal.pntd.0003258. eCollection 2014. PLoS Negl Trop Dis. 2014. PMID: 25412435 Free PMC article. Review.
-
Protective or Detrimental? Understanding the Role of Host Immunity in Leishmaniasis.Microorganisms. 2019 Dec 13;7(12):695. doi: 10.3390/microorganisms7120695. Microorganisms. 2019. PMID: 31847221 Free PMC article. Review.
Cited by
-
Severe mucosal leishmaniasis with torpid and fatal evolution.Clin Case Rep. 2022 Aug 14;10(8):e6220. doi: 10.1002/ccr3.6220. eCollection 2022 Aug. Clin Case Rep. 2022. PMID: 35990382 Free PMC article.
-
Therapeutic response and safety of the topical, sequential use of antiseptic, keratolytic, and pentamidine creams (3-PACK) on Leishmania (Viannia) braziliensis-infected mice.Mem Inst Oswaldo Cruz. 2019;114:e180535. doi: 10.1590/0074-02760180535. Epub 2019 May 13. Mem Inst Oswaldo Cruz. 2019. PMID: 31090861 Free PMC article.
-
Commentary on the Issue of Leishmania Infection: Focus on Some Pathogenetic, Clinical, and Epidemiological Aspects.Vet Sci. 2025 Jun 1;12(6):536. doi: 10.3390/vetsci12060536. Vet Sci. 2025. PMID: 40559773 Free PMC article.
-
Is There Any Difference in the In Situ Immune Response in Active Localized Cutaneous Leishmaniasis That Respond Well or Poorly to Meglumine Antimoniate Treatment or Spontaneously Heal?Microorganisms. 2023 Jun 22;11(7):1631. doi: 10.3390/microorganisms11071631. Microorganisms. 2023. PMID: 37512804 Free PMC article.
-
Dual Role of Insulin-Like Growth Factor (IGF)-I in American Tegumentary Leishmaniasis.J Immunol Res. 2021 Mar 29;2021:6657785. doi: 10.1155/2021/6657785. eCollection 2021. J Immunol Res. 2021. PMID: 33860062 Free PMC article.
References
-
- Adaui V., Lye L. F., Akopyants N. S., Zimic M., Llanos-Cuentas A., Garcia L., et al. (2016). Association of the endobiont double-stranded RNA virus LRV1 with treatment failure for human Leishmaniasis Caused by Leishmania braziliensis in Peru and Bolivia. J. Infect. Dis. 213 112–121. 10.1093/infdis/jiv354 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources