

Molecular subtype predicts incidence and prognosis of brain metastasis from breast cancer in SEER database
- PMID: 29971531
- PMCID: PMC11813522
- DOI: 10.1007/s00432-018-2697-2
Molecular subtype predicts incidence and prognosis of brain metastasis from breast cancer in SEER database
Abstract
Purpose: To evaluate the impact of molecular subtype on incidence and prognosis of brain metastasis from breast cancer.
Methods: The Surveillance, Epidemiology, and End Results (SEER) 18 registry was used to select breast cancer patients from 2010 to 2014. Molecular subtypes were classified as luminal A (hormone receptor [HR]+/human epidermal growth factor receptor 2 [HER2]-), luminal B (HR+/HER2+), HER2 (HR-/HER2+), or triple negative breast cancer (TNBC) (HR-/HER2-). The incidence and prognosis of brain metastasis was evaluated according to molecular subtype.
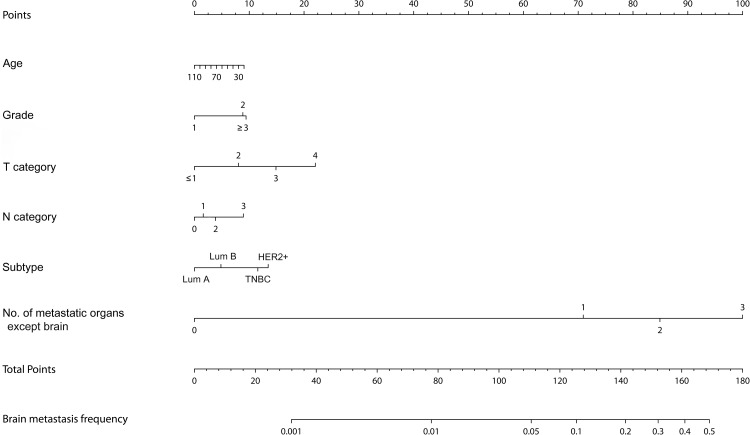
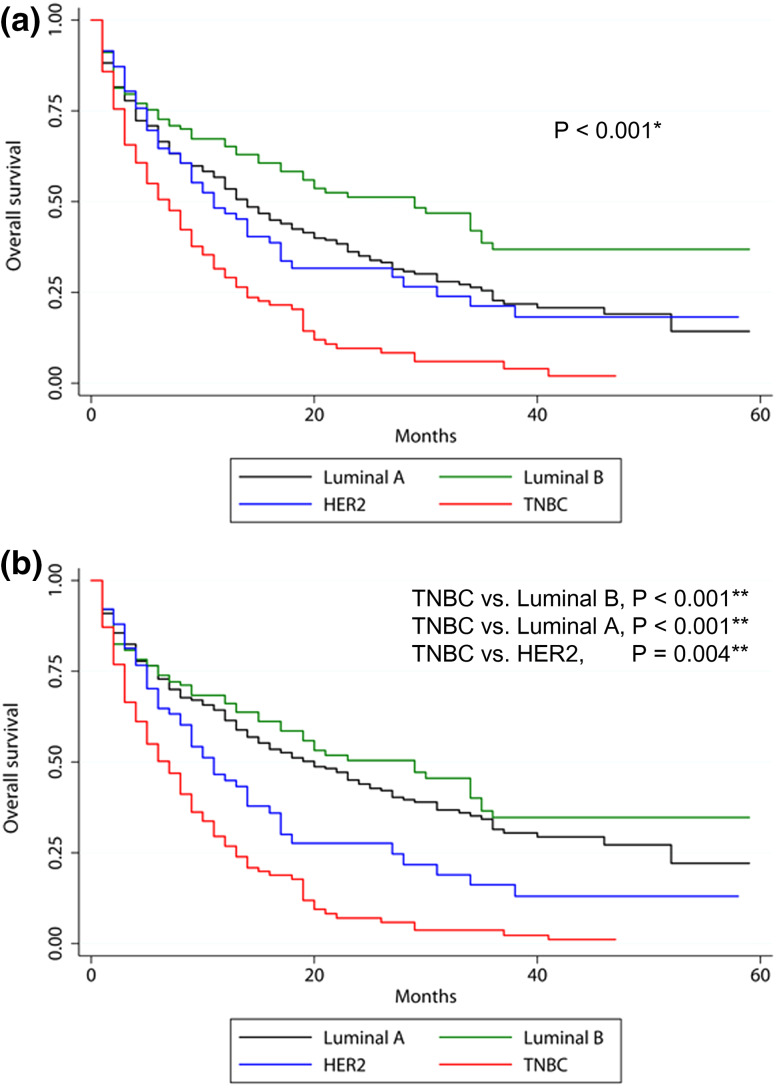
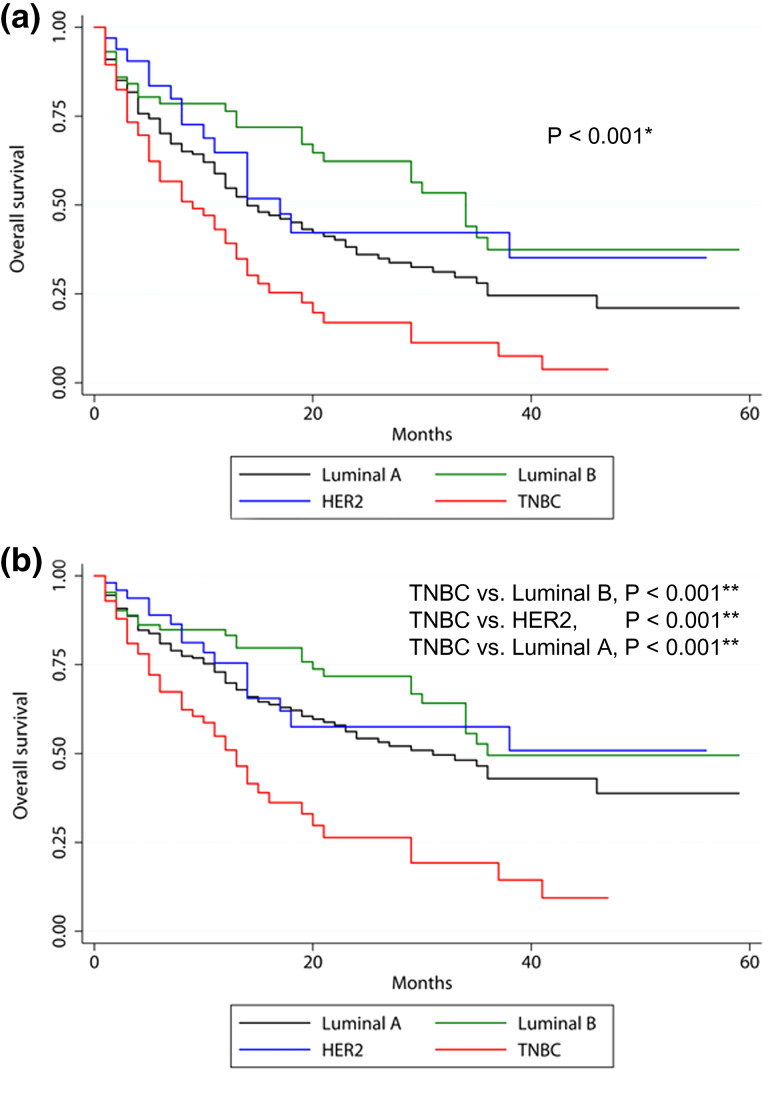
Results: Among the 206913 breast cancer patients, the HER2 subtype showed the highest incidence of brain metastasis (1.0%). HER2 and TNBC with multiple extracranial metastases (bone, liver, and lung) showed a high incidence of brain metastasis (28.0 and 30.8%, respectively). Median survival of luminal A, luminal B, HER2, and TNBC in brain metastasis was 12, 23, 10, and 6 months (p < 0.001), and in brain metastasis without visceral metastasis was 14, 34, 17, and 8 months (p < 0.001). On multivariate analysis, the order of subtype by favorable prognosis was luminal B, luminal A, HER2, and TNBC in all brain metastasis, while for brain metastasis patients without visceral metastasis, the order was luminal B, HER2, luminal A, and TNBC.
Conclusions: Molecular subtype and visceral metastasis should be considered for prediction of prognosis for patients with brain metastasis. The patients with HER2 and TNBC cancer subtypes having visceral metastasis, close surveillance could contribute to early detection of brain metastasis and may putatively lead to improved quality of life and survival.
Keywords: Brain metastasis; Breast cancer; Incidence; Molecular subtype; Prognosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
