

Subtypes of pediatric acute respiratory distress syndrome have different predictors of mortality
- PMID: 29971591
- PMCID: PMC6460461
- DOI: 10.1007/s00134-018-5286-6
Subtypes of pediatric acute respiratory distress syndrome have different predictors of mortality
Abstract
Purpose: Acute respiratory distress syndrome (ARDS) is heterogeneous in etiology, which may affect outcomes. Stratification into biologically-defined subtypes may reduce heterogeneity. However, it is unknown whether pediatric ARDS has clinically relevant subtypes. We aimed to determine whether clinical characteristics and predictors of mortality differed between direct and indirect ARDS, and separately between infectious and non-infectious ARDS.
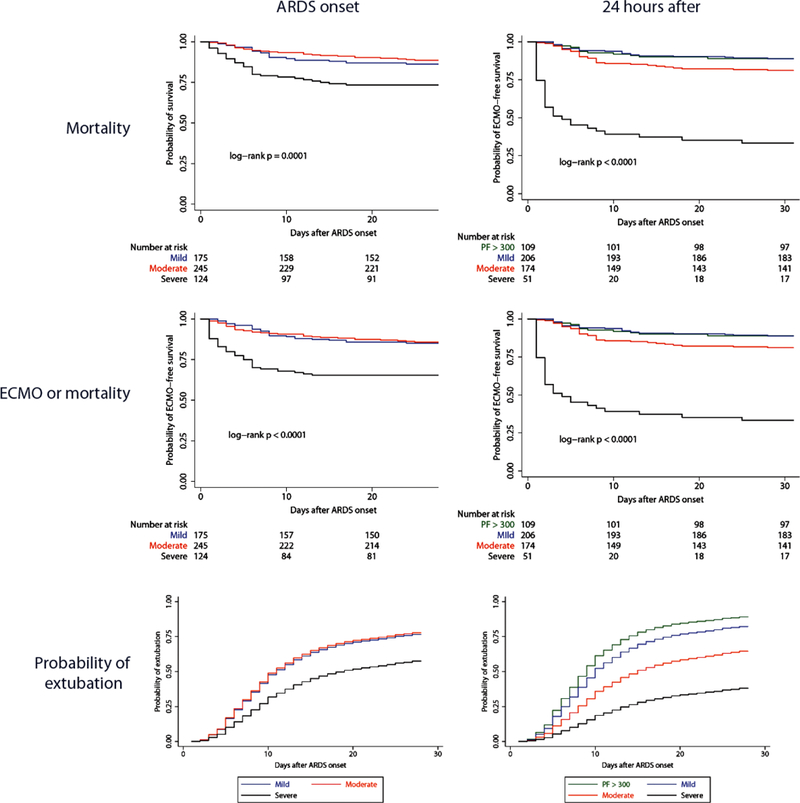
Methods: This was a single center, prospective cohort study of 544 children with ARDS (Berlin) between July 2011 and June 2017, stratified into direct versus indirect ARDS, and separately into infectious versus non-infectious ARDS. Multiple logistic regression was used to test for predictors of mortality in the entire cohort, and separately within subtypes. Effect modification by subtype was assessed using interaction tests.
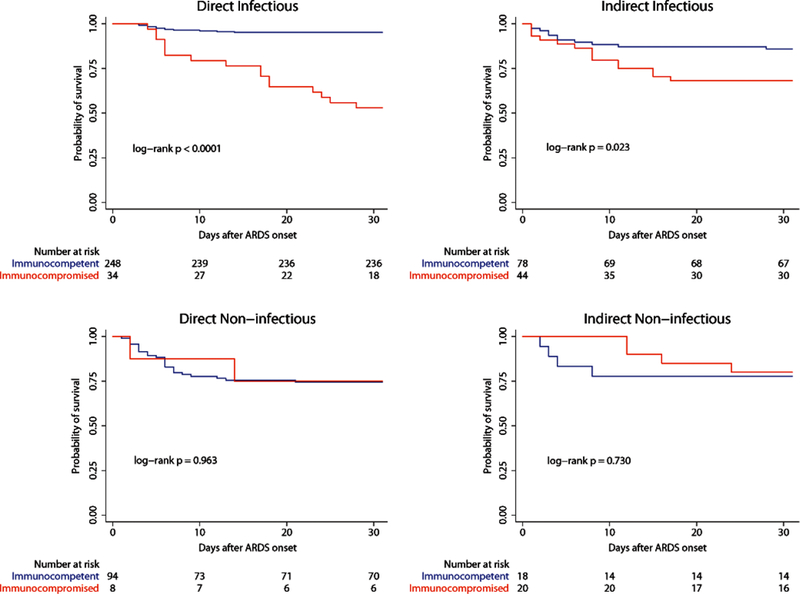
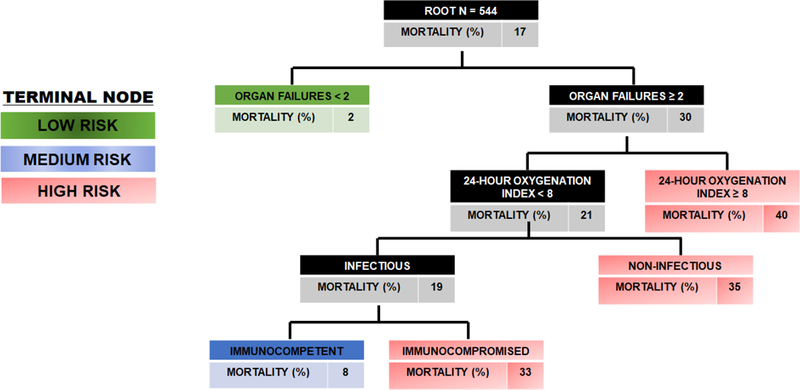
Results: Direct ARDS had lower severity of illness (p < 0.001) but worse oxygenation (p < 0.001), relative to indirect. Predictors of mortality were similar for direct and indirect ARDS. When comparing infectious and non-infectious ARDS, infectious ARDS had lower severity of illness (p < 0.001), worse oxygenation (p = 0.014), and lower mortality (p = 0.013). In multivariable analysis, immunocompromised status demonstrated effect modification between infectious and non-infectious ARDS (p = 0.005 for interaction), with no association with mortality in non-infectious ARDS.
Conclusions: In children, direct and indirect ARDS have distinct clinical characteristics, but similar outcomes and similar predictors of mortality. In contrast, infectious and non-infectious ARDS demonstrate heterogeneity of clinical characteristics, mortality, and predictors of mortality, with traditional predictors of ARDS mortality only applicable to infectious ARDS.
Keywords: ARDS; Children; Direct ARDS; Infectious ARDS; PARDS.
Conflict of interest statement
CONFLICTS OF INTEREST
Dr. Yehya’s institution receives funding from the NIH (K12-HL-136688). Dr. Thomas reports personal fees from Therabron and Carefusion, all outside of the submitted work.
Figures
Comment in
-
Use of time-varying coefficients in a Cox regression model when the proportional hazard assumption is violated.Intensive Care Med. 2018 Nov;44(11):2017-2019. doi: 10.1007/s00134-018-5351-1. Epub 2018 Aug 27. Intensive Care Med. 2018. PMID: 30151689 No abstract available.
-
Heterogeneity of Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2020 Mar 15;201(6):728-730. doi: 10.1164/rccm.201906-1110RR. Am J Respir Crit Care Med. 2020. PMID: 31995400 No abstract available.
References
-
- Willson DF, Truwit JD, Conaway MR, Traul CS, Egan EE, (2015) The Adult Calfactant in Acute Respiratory Distress Syndrome Trial. Chest 148: 356–364 - PubMed
-
- National Heart L, Blood Institute ACTN, Truwit JD, Bernard GR, Steingrub J, Matthay MA, Liu KD, Albertson TE, Brower RG, Shanholtz C, Rock P, Douglas IS, deBoisblanc BP, Hough CL, Hite RD, Thompson BT, (2014) Rosuvastatin for sepsis-associated acute respiratory distress syndrome. N Engl J Med 370: 2191–2200 - PMC - PubMed
-
- Mrozek S, Jabaudon M, Jaber S, Paugam-Burtz C, Lefrant JY, Rouby JJ, Asehnoune K, Allaouchiche B, Baldesi O, Leone M, Lu Q, Bazin JE, Roszyk L, Sapin V, Futier E, Pereira B, Constantin JM, Azurea n, (2016) Elevated Plasma Levels of sRAGE Are Associated With Nonfocal CT-Based Lung Imaging in Patients With ARDS: A Prospective Multicenter Study. Chest 150: 998–1007 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
