

The impact of heart, lung and diaphragmatic ultrasound on prediction of failed extubation from mechanical ventilation in critically ill patients: a prospective observational pilot study
- PMID: 29971618
- PMCID: PMC6029991
- DOI: 10.1186/s13089-018-0096-1
The impact of heart, lung and diaphragmatic ultrasound on prediction of failed extubation from mechanical ventilation in critically ill patients: a prospective observational pilot study
Abstract
Background: Failed extubation from mechanical ventilation in critically ill patients is multifactorial, complex and not well understood. We aimed to identify whether combined transthoracic echocardiography, lung and diaphragmatic ultrasound can predict extubation failure in critically ill patients.
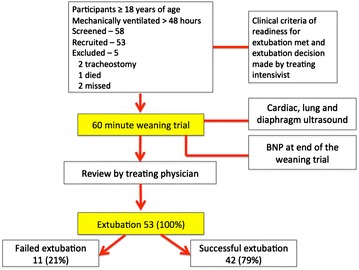
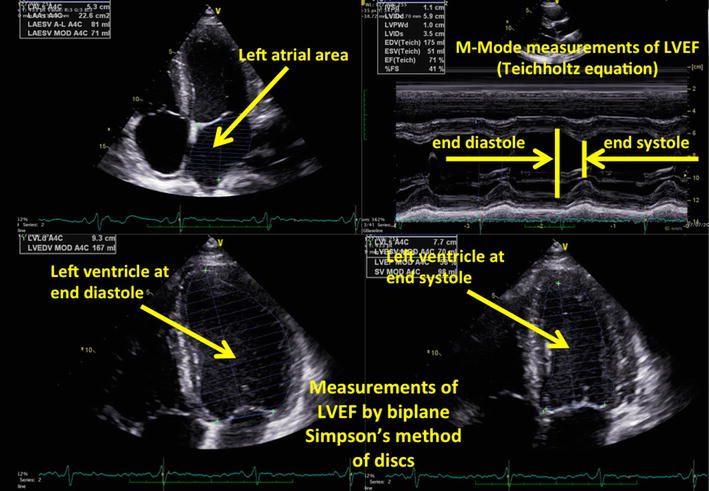
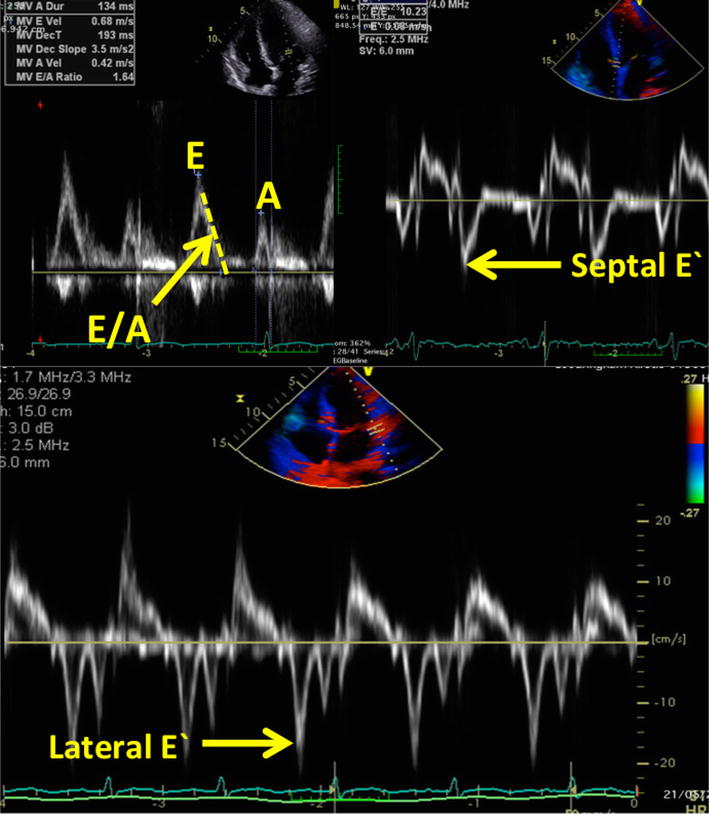
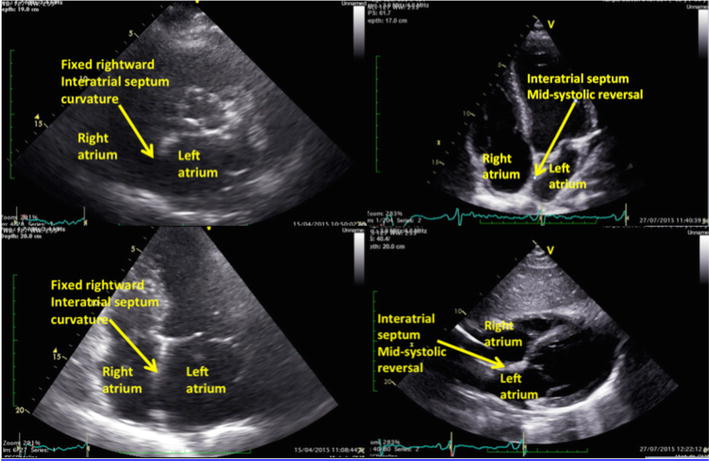
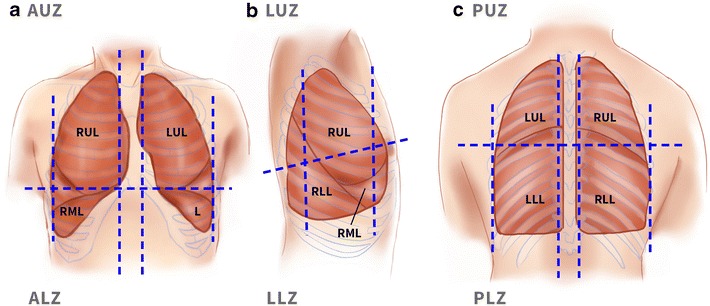
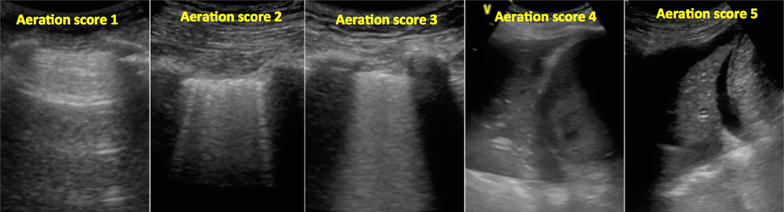
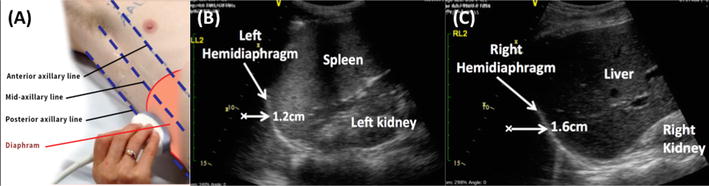
Results: Fifty-three participants who were intubated > 48 h and deemed by the treating intensivist ready for extubation underwent a 60-min pre-extubation weaning trial (pressure support ≤ 10 cmH2O and positive end expiratory pressure 5 cmH2O). Prior to extubation, data collected included ultrasound assessment of left ventricular ejection fraction, left atrial area, early diastolic trans-mitral flow velocity wave (E), early diastolic trans-mitral flow velocity wave/late diastolic trans-mitral flow velocity wave (E/A), early diastolic trans-mitral flow velocity wave/early diastolic mitral annulus velocity (E/E'), interatrial septal motion, lung loss of aeration score and diaphragm movement. At the end of the weaning trial, the rapid shallow breathing index and serum B-type natriuretic peptide concentration were measured. Success and failure of weaning was assessed by defined criteria. Decision to extubate was at the discretion of the treating intensivist. Failure of extubation was defined as re-intubation, non-invasive ventilation or death within 48 h after extubation. Of 53 extubated participants, 11 failed extubation. Failed extubation was associated with diabetes, ischaemic heart disease, higher E/E' (OR 1.27, 95% CI 1.05-1.54), left atrial area (OR 1.14, CI 1.02-1.28), fixed rightward curvature of the interatrial septum (OR 12.95, CI 2.73-61.41), and higher loss of aeration score of anterior and lateral regions of the lungs (OR 1.41, CI 1.01-1.82).
Conclusions: Failed extubation in mechanically ventilated patients is more prevalent if markers of left ventricular diastolic dysfunction and loss of lung aeration are present.
Keywords: Diaphragm; Echocardiography; Lung; RSBI; Ultrasound; Weaning.
Figures
References
-
- Esteban A, Alia I, Tobin MJ, Gil A, Gordo F, Vallverdu I, et al. Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1999;159(2):512–518. doi: 10.1164/ajrccm.159.2.9803106. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
