

Mandatory criteria for the application of variability-based parameters of fluid responsiveness: a prospective study in different groups of ICU patients
- PMID: 29971990
- PMCID: PMC6052358
- DOI: 10.1631/jzus.B1700243
Mandatory criteria for the application of variability-based parameters of fluid responsiveness: a prospective study in different groups of ICU patients
Abstract
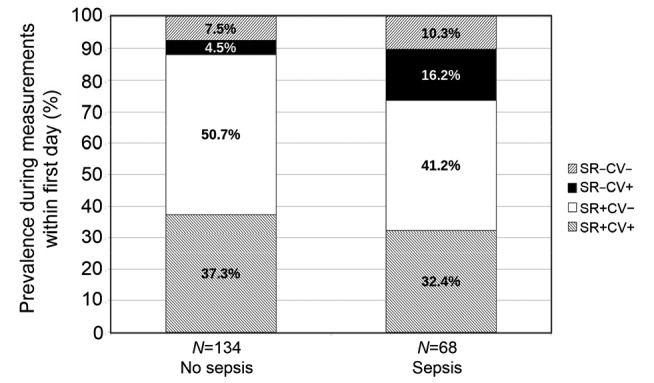
Background and objective: Stroke volume variation (SVV) has high sensitivity and specificity in predicting fluid responsiveness. However, sinus rhythm (SR) and controlled mechanical ventilation (CV) are mandatory for their application. Several studies suggest a limited applicability of SVV in intensive care unit (ICU) patients. We hypothesized that the applicability of SVV might be different over time and within certain subgroups of ICU patients. Therefore, we analysed the prevalence of SR and CV in ICU patients during the first 24 h of PiCCO-monitoring (primary endpoint) and during the total ICU stay. We also investigated the applicability of SVV in the subgroups of patients with sepsis, cirrhosis, and acute pancreatitis.
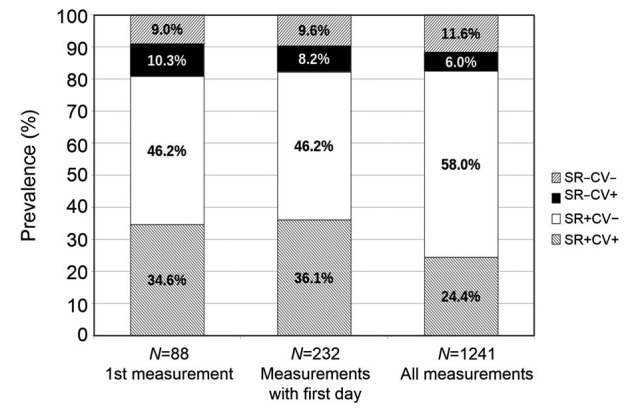
Methods: The prevalence of SR and CV was documented immediately before 1241 thermodilution measurements in 88 patients.
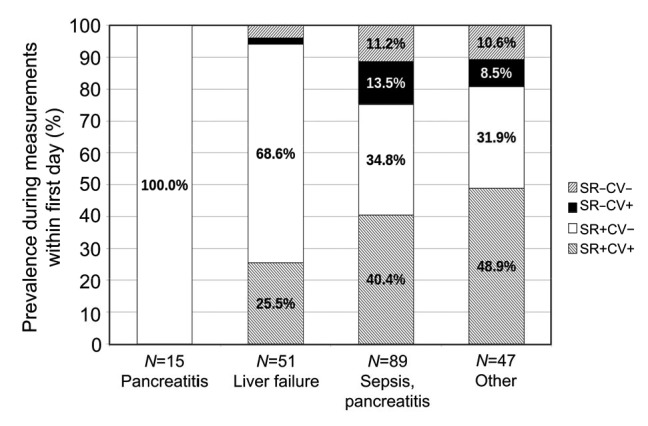
Results: In all measurements, SVV was applicable in about 24%. However, the applicability of SVV was time-dependent: the prevalence of both SR and CV was higher during the first 24 h compared to measurements thereafter (36.1% vs. 21.9%; P<0.001). Within different subgroups, the applicability during the first 24 h of monitoring ranged between 0% in acute pancreatitis, 25.5% in liver failure, and 48.9% in patients without pancreatitis, liver failure, pneumonia or sepsis.
Conclusions: The applicability of SVV in a predominantly medical ICU is only about 25%-35%. The prevalence of both mandatory criteria decreases over time during the ICU stay. Furthermore, the applicability is particularly low in patients with acute pancreatitis and liver failure.
Keywords: Hemodynamic monitoring; Preload; Fluid responsiveness; Stroke volume variation; Pulse pressure variation.
Conflict of interest statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). The need for informed consent was waived due to the observational approach of the study.
Figures
References
-
- Benes J, Zatloukal J, Kletecka J, et al. Respiratory induced dynamic variations of stroke volume and its surrogates as predictors of fluid responsiveness: applicability in the early stages of specific critical states. J Clin Monit Comput. 2014;28(3):225–231. doi: 10.1007/s10877-013-9524-8. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
