

Major Changes of von Willebrand Factor Multimer Distribution in Cirrhotic Patients with Stable Disease or Acute Decompensation
- PMID: 29972862
- PMCID: PMC6202934
- DOI: 10.1055/s-0038-1661393
Major Changes of von Willebrand Factor Multimer Distribution in Cirrhotic Patients with Stable Disease or Acute Decompensation
Abstract
Background: There is an unstable balance between pro- and anti-haemostatic processes in patients with cirrhosis. We hypothesized, that in patients with acute decompensation (AD) the major alterations of von Willebrand factor (VWF) could contribute to the pro-thrombotic situation as compared to patients with stable (ST) cirrhosis.
Patients and methods:
We analysed different parameters of VWF, including detailed multimer distribution by densitometry and platelet adhesion, together with
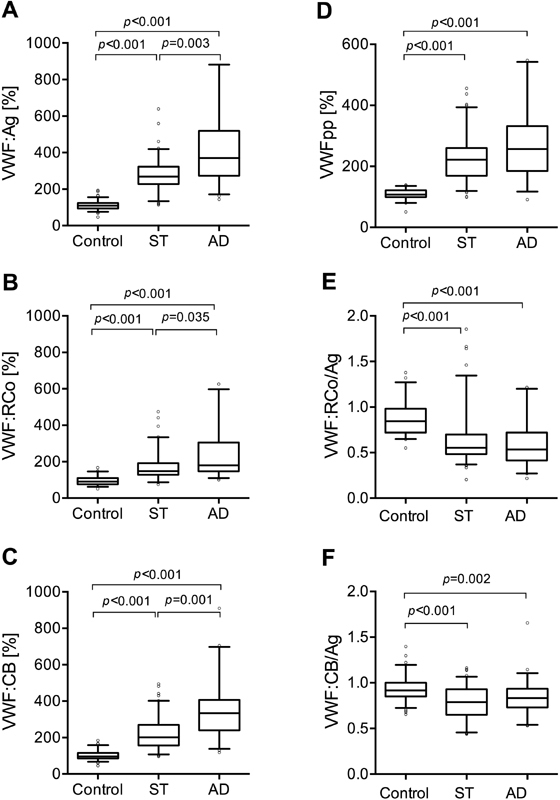
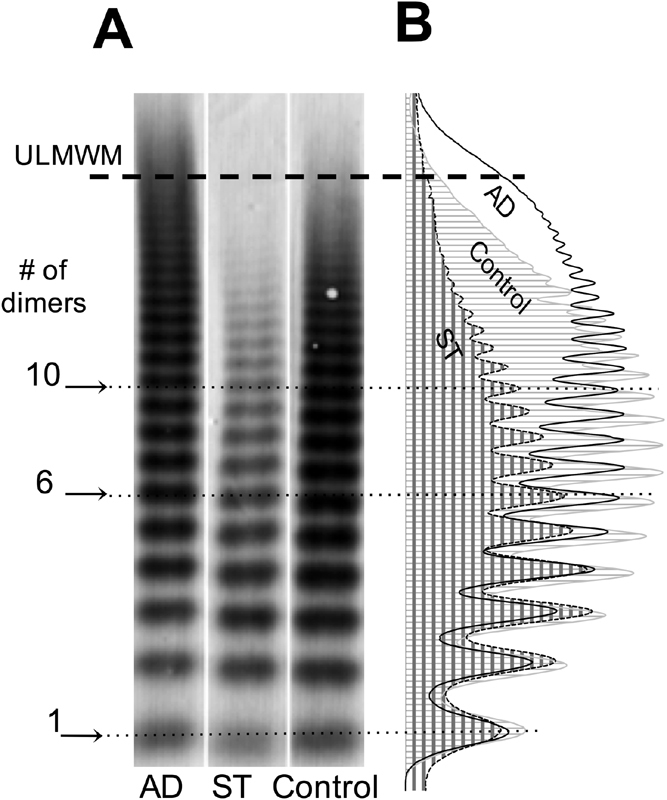
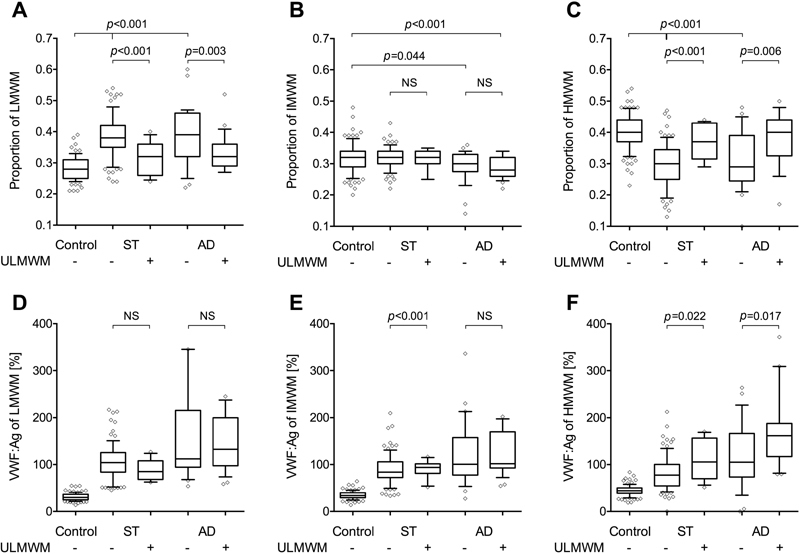
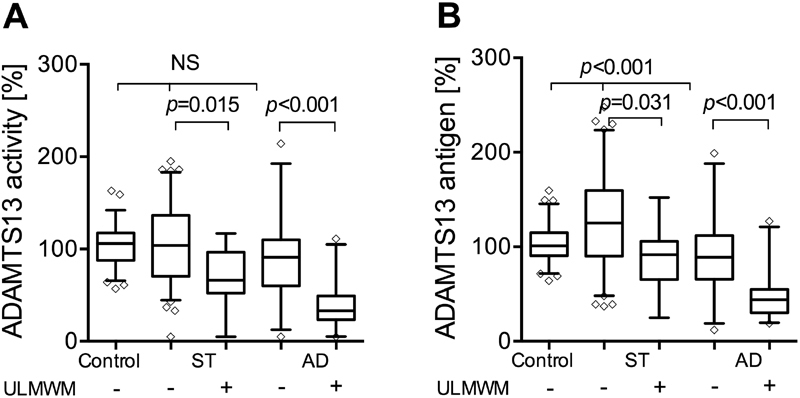
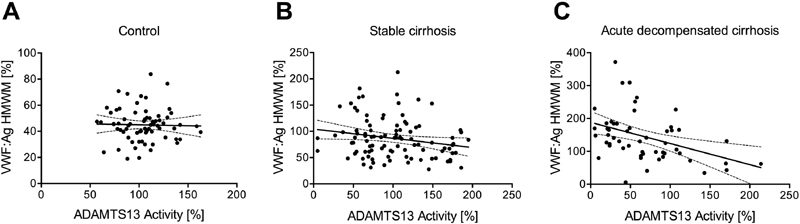
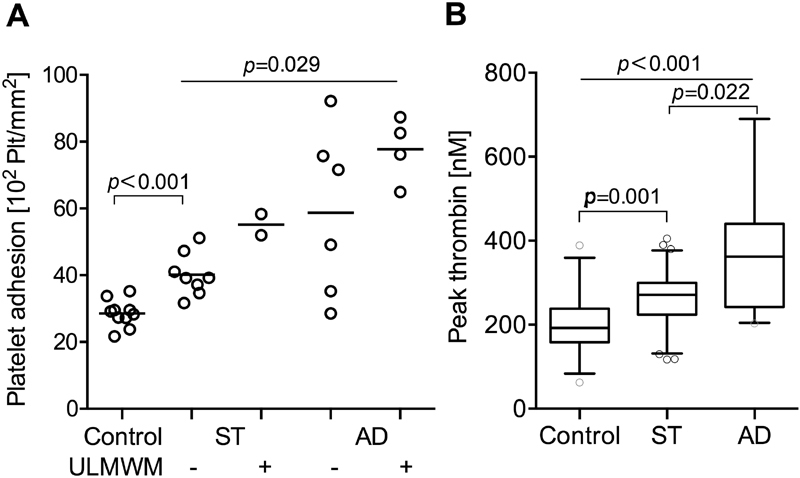
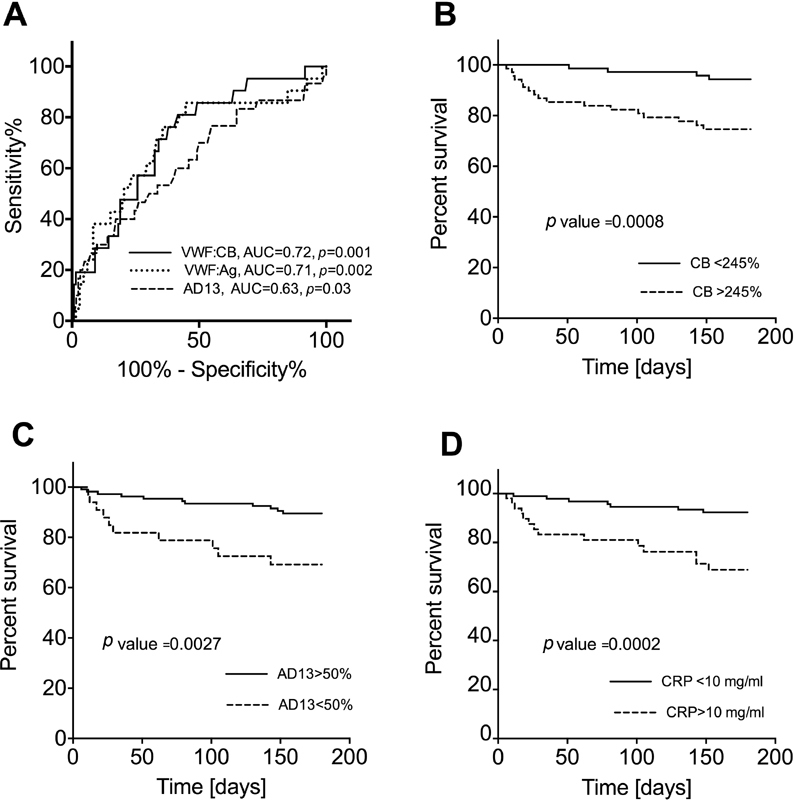
Results: VWF antigen, ristocetin co-factor as well as collagen-binding activities were elevated in both cirrhotic groups in a stepwise manner. There was a decrease in high and an increase in low molecular weight multimer ratios in the majority of ST cirrhosis. However, in 24 out of 54 AD patients, ultra-large VWF multimers (ultra-large molecular weight multimers [ULMWM]) were found. ADAMTS13 activity in ST and AD patients without ULMWM was similar to controls (median [interquartile range; IQR]%: 98 [67-132] and 91 [60-110] vs. 106 [88-117], respectively). The presence of ULMWM in AD patients was associated with low ADAMTS13 activity [33 (24-49)%] and high CRP level [23 (7.1-83.6) mg/L]. Adhesion of normal platelets showed a stepwise increase in the presence of cirrhotic plasmas, reaching the highest level in AD patients with ULMWM.
Conclusion: Characteristic changes of VWF parameters are seen in ST cirrhosis. In AD patients, highly increased VWF and reduced ADAMTS13 activity could be found, along with the presence of ULMWM, which are possible markers and contributors of the disease progression.
Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
None.
Figures
References
-
- Tripodi A. Liver disease and hemostatic (dys)function. Semin Thromb Hemost. 2015;41(05):462–467. - PubMed
-
- Lisman T, Porte R J. Rebalanced hemostasis in patients with liver disease: evidence and clinical consequences. Blood. 2010;116(06):878–885. - PubMed
-
- Lisman T, Bongers T N, Adelmeijer J et al. Elevated levels of von Willebrand Factor in cirrhosis support platelet adhesion despite reduced functional capacity. Hepatology. 2006;44(01):53–61. - PubMed
-
- La Mura V, Reverter J C, Flores-Arroyo A et al. Von Willebrand factor levels predict clinical outcome in patients with cirrhosis and portal hypertension. Gut. 2011;60(08):1133–1138. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
