

What is impact of nonsteroidal anti-inflammatory drugs in the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a meta-analysis of randomized controlled trials
- PMID: 29973142
- PMCID: PMC6032784
- DOI: 10.1186/s12876-018-0837-4
What is impact of nonsteroidal anti-inflammatory drugs in the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a meta-analysis of randomized controlled trials
Abstract
Background: Recently, although studies have investigated the role of NSAIDs in the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP), selection of the ideal drug, the time and route of its administration for the appropriate population remain controversial.
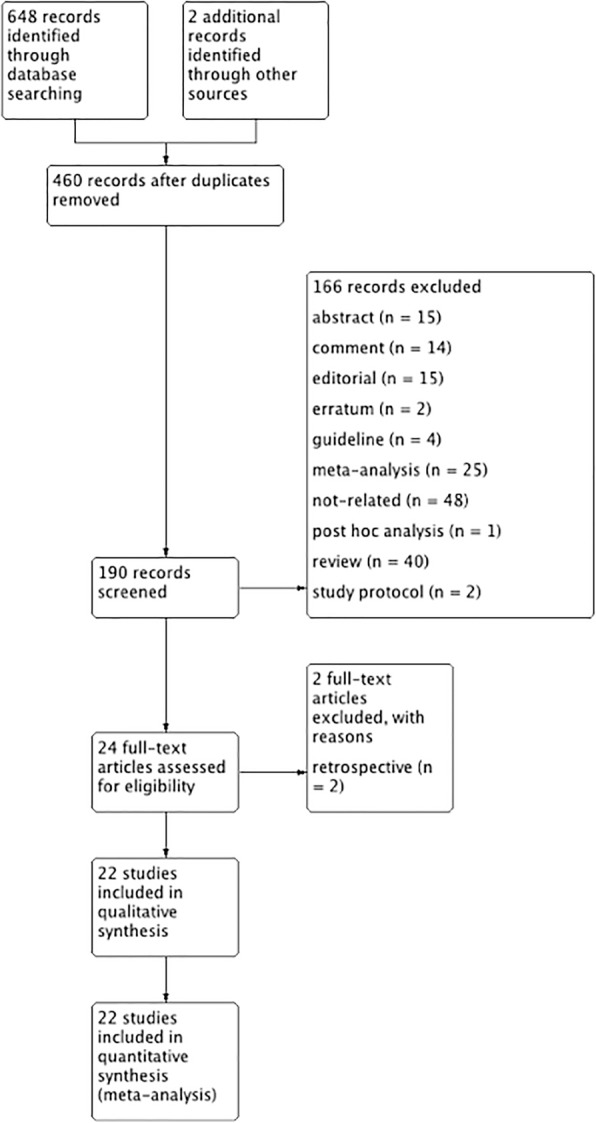
Methods: A systematic search was done in sources including PubMed, Embase, Web of Science, the Cochrane Library Central, and ClinicalTrials.gov from from August 1, 1990 to August 1, 2017. Randomized controlled trials comparing the prophylactic use of NSAIDs versus a placebo were included. Statistical analysis was performed using the RevMan 5.3 software to assess the outcomes.
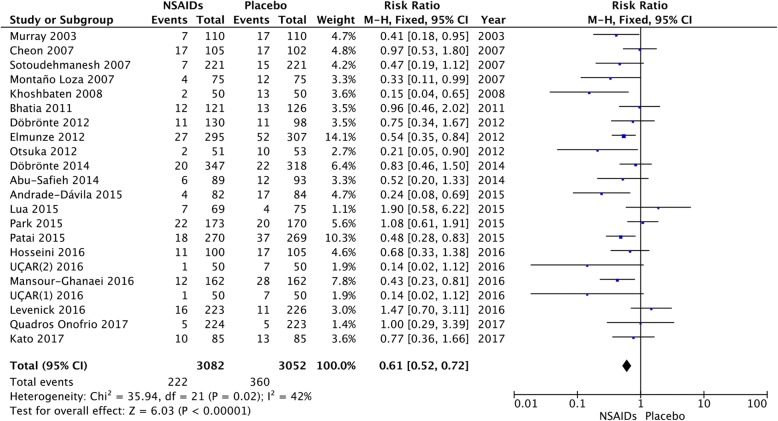
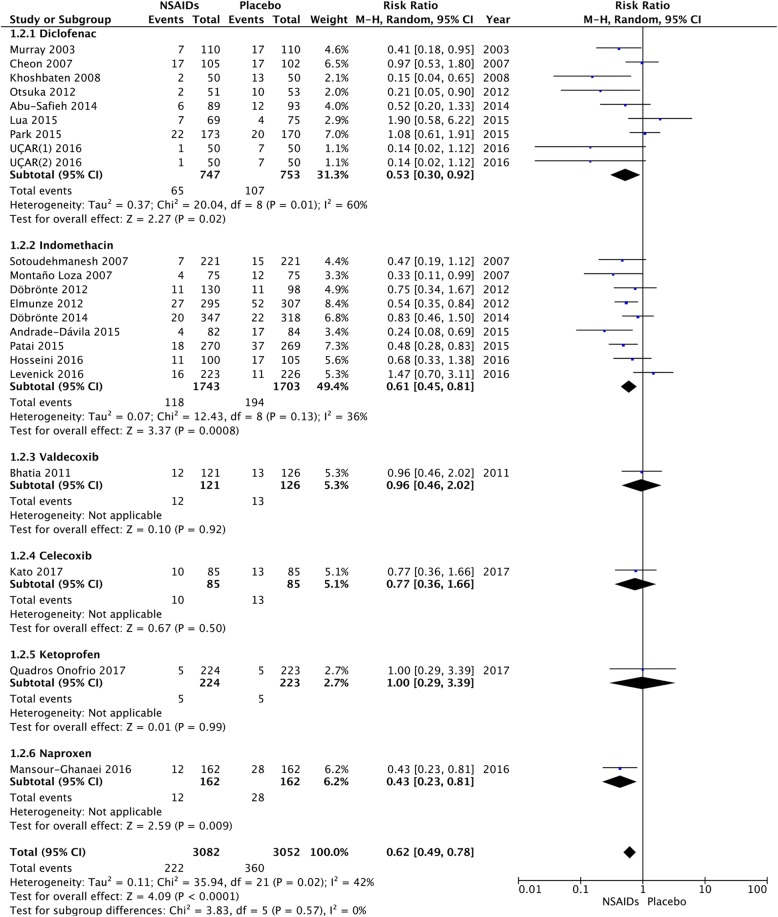
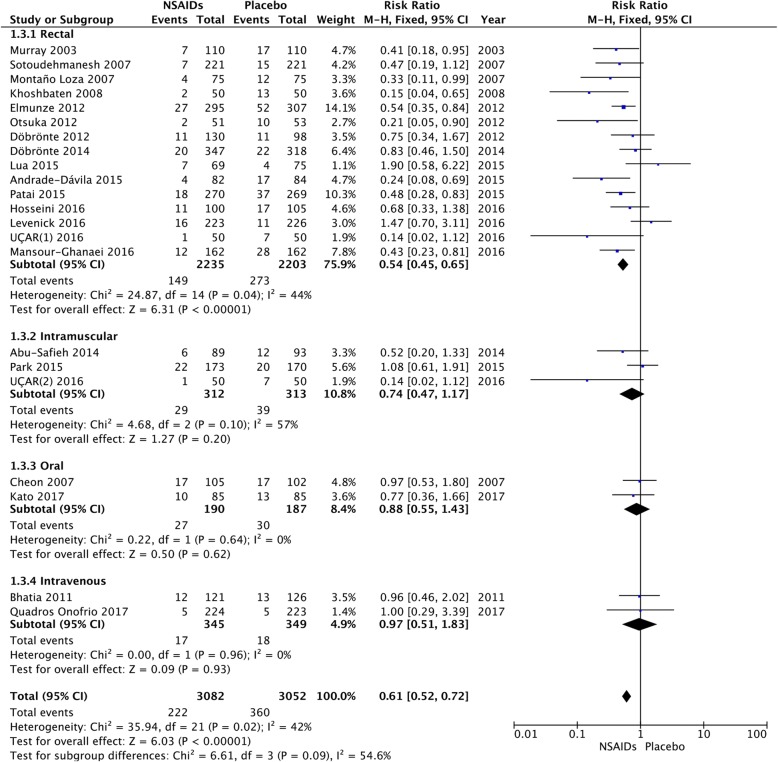
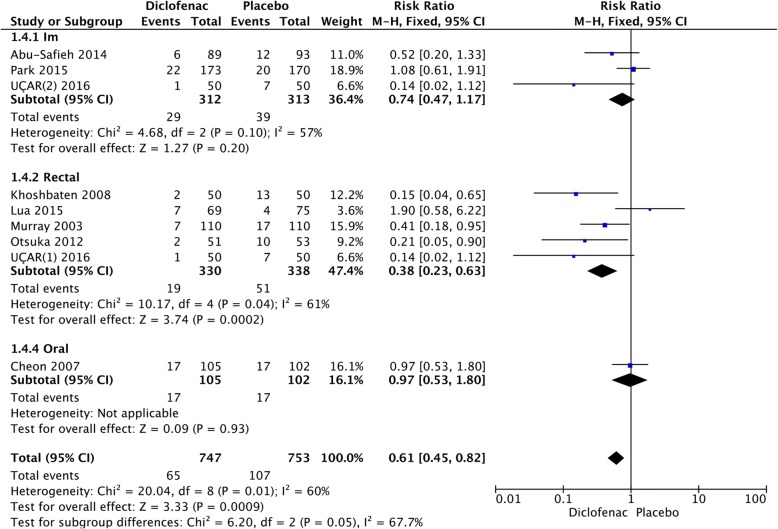
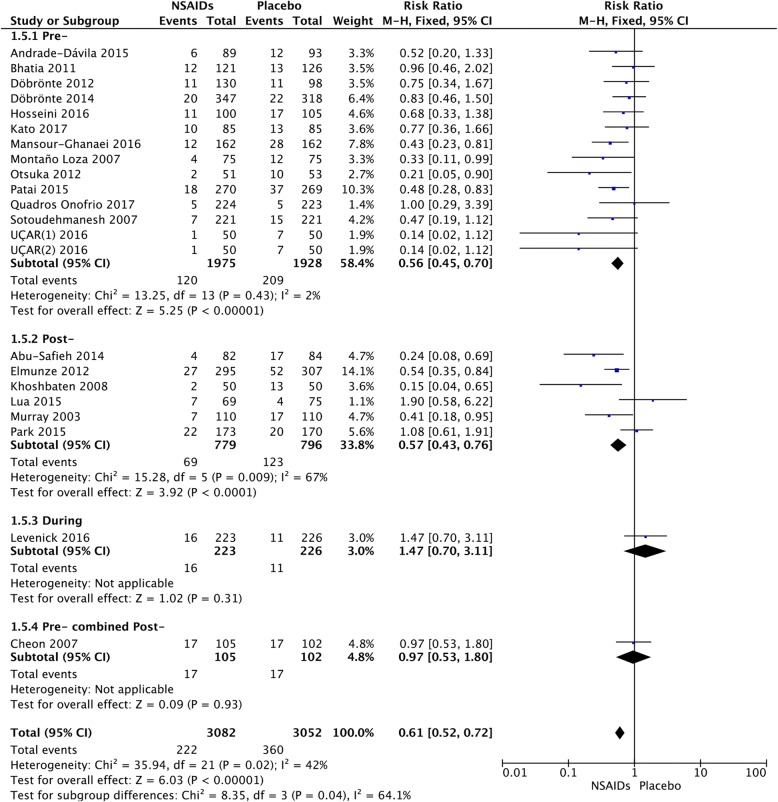
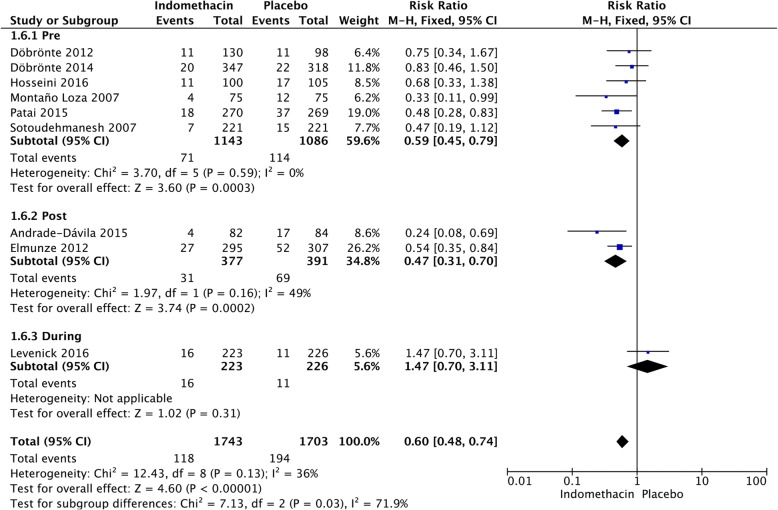
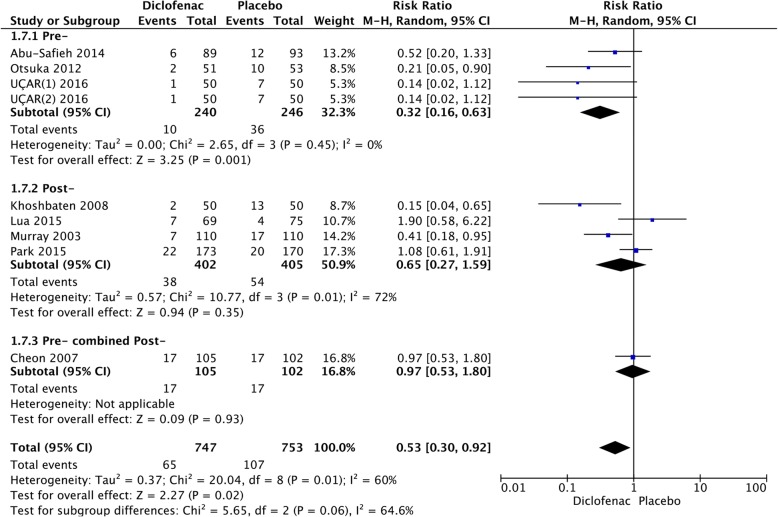
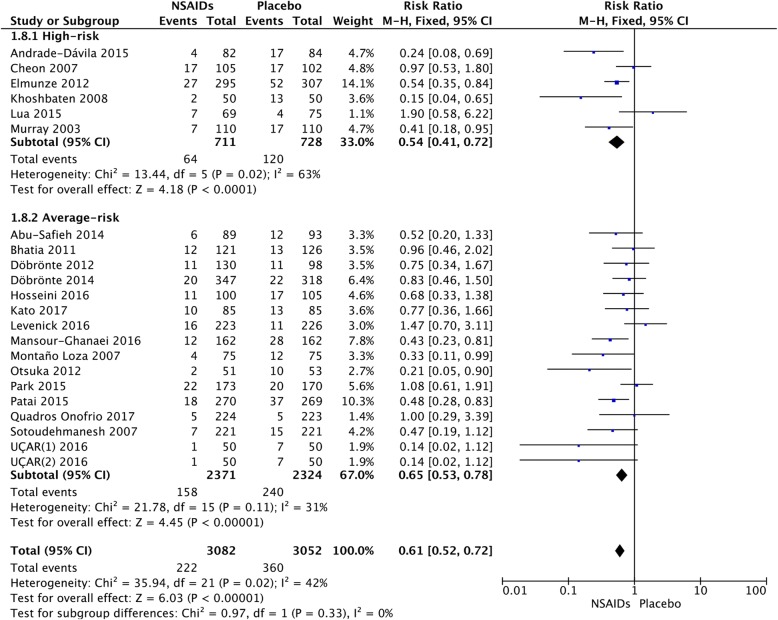
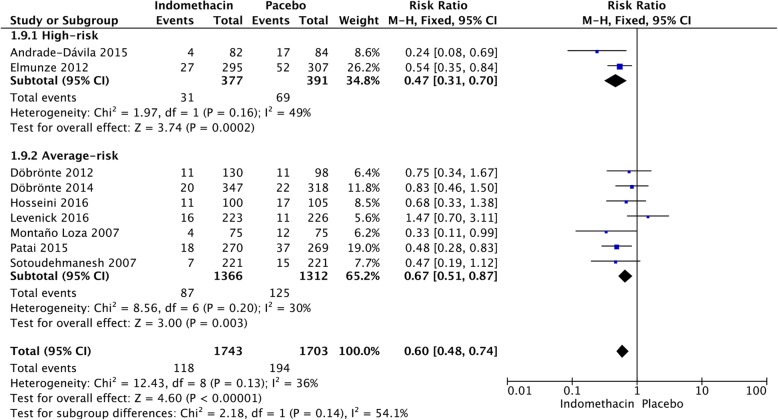
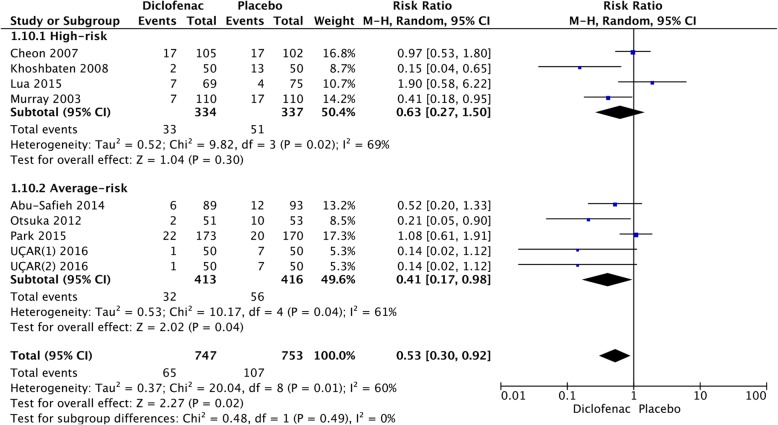
Results: A total of 21 randomized controlled trials were included in the meta-analysis. Our study showed that NSAIDs significantly reduced the incidence of PEP (RR, 0.61, 95%CI,0.52-0.72; p < 0.00001). The analysis showed that indomethacin administration post-ERCP (RR, 0.47; 95% CI, 0.31-0.70; p = 0.0002) appeared to be more effective in preventing PEP than indomethacin administration pre-ERCP (RR, 0.59; 95% CI, 0.45-0.79; P = 0.0003), but there was no significant difference between the high-risk and average-risk population(p = 0.13). In the diclofenac group, it was noted that administration of diclofenac pre-ERCP (RR, 0.32; 95% CI, 0.16-0.63; p = 0.001) was more effective than that in post-ERCP (RR, 0.65; 95% CI, 0.27-1.599; p = 0.35). The relative risk of PEP was 0.63 (95% CI, 0.27-1.50; p = 0.30) in high-risk patients and 0.41 (95% CI, 0.17-0.98; p = 0.02) in average-risk patients. With regard to the route of administration, PEP decreased significantly only in patients receiving the drug rectally (RR, 0.53; 95% CI, 0.44-0.63; p < 0.00001), but not for those who received intramuscularly (RR, 0.74; 95% CI, 0.47-1.17; p = 0.20), intravenously (RR, 0.97; 95% CI, 0.51-1.83; p = 0.93), and orally (RR = 0.88; 95% CI, 0.55-0.1.43; p = 0.62).
Conclusions: Rectal administration of NSAIDs (both indomethacin and diclofenac) was effective in preventing PEP in unselected patients. A single dose of indomethacin after ERCP might be effective in preventing PEP in both high-risk and average-risk patients. However, diclofenac administered rectally before ERCP might be protective against PEP in high-risk patients compared to a placebo. However, more high quality head-to-head RCTs are required.
Keywords: Diclofenac; ERCP; Indomethacin; Meta-analysis; NSAIDs; Pancreatitis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
