

An atypical presentation of high potassium renal secretion rate in a patient with thyrotoxic periodic paralysis: a case report
- PMID: 29973184
- PMCID: PMC6031107
- DOI: 10.1186/s12882-018-0971-9
An atypical presentation of high potassium renal secretion rate in a patient with thyrotoxic periodic paralysis: a case report
Abstract
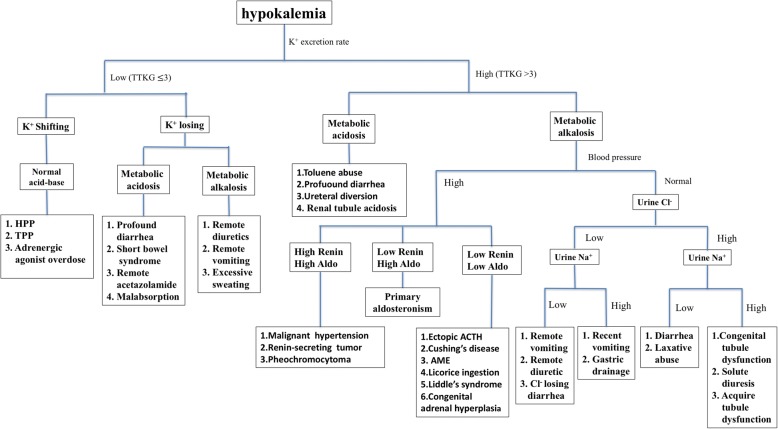
Background: Hypokalemia is one of the most common clinical electrolyte imbalance problems, and thyrotoxic periodic paralysis (TPP) is a leading cause of presentation to the emergency department. Low renal potassium secretion rates, a normal acid-base balance in the blood, and hyperthyroidism are the hallmarks of suspected TPP.
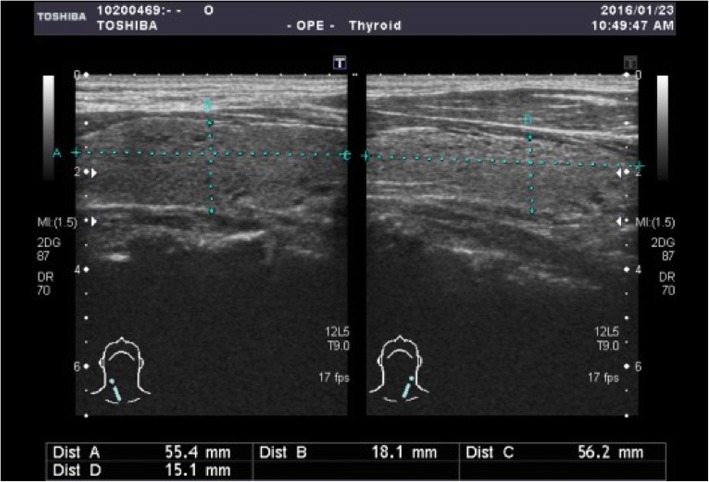
Case presentation: Here we report the case of a 36-year-old man who presented to the emergency department with a sudden onset of acute muscle weakness at 5 h prior to admission. Biochemistry tests revealed hypokalemia with hyperthyroidism and renal potassium wasting. TPP was initially not favored due to the presence of renal potassium wasting. However, his serum potassium level rebounded rapidly within several hours after potassium supplementation, indicating that the intracellular shifting of potassium ions was the main etiology for his hypokalemia. The early stage of TPP development may have contributed to this paradox.
Conclusion: Therefore, it is premature to rule out TPP based on the presentation of high renal potassium secretion rates alone. This finding may result in an incorrect impression being made in the early stage of TTP and may consequently lead to an inappropriate potassium supplementation policy.
Keywords: Hyperthyroidism; Hypokalemia; Paralysis; Renal potassium wasting; Thyrotoxic periodic paralysis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for this publication of laboratory information and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Hypokalemic Paralysis Complicated by Concurrent Hyperthyroidism and Hyperaldosternoism: A Case Report.Am J Case Rep. 2017 Jan 4;18:12-16. doi: 10.12659/ajcr.901793. Am J Case Rep. 2017. PMID: 28050008 Free PMC article.
-
Thyrotoxic periodic paralysis associated with lactic metabolic acidosis: Case report of an African man and review of literature.Ann Endocrinol (Paris). 2023 Aug;84(4):440-445. doi: 10.1016/j.ando.2023.01.007. Epub 2023 Feb 8. Ann Endocrinol (Paris). 2023. PMID: 36758896 Review.
-
Clinical review: Thyrotoxic periodic paralysis: a diagnostic challenge.J Clin Endocrinol Metab. 2006 Jul;91(7):2490-5. doi: 10.1210/jc.2006-0356. Epub 2006 Apr 11. J Clin Endocrinol Metab. 2006. PMID: 16608889 Review.
-
Case report: thyrotoxic periodic paralysis, an unusual cause of hypokalemia.Acta Clin Belg. 2024 Jun;79(3):225-228. doi: 10.1080/17843286.2024.2365491. Epub 2024 Jun 13. Acta Clin Belg. 2024. PMID: 38869234
-
Lower-Extremity Weakness in a Teenager Due to Thyrotoxic Periodic Paralysis.J Emerg Med. 2017 Apr;52(4):e133-e137. doi: 10.1016/j.jemermed.2016.11.006. Epub 2016 Dec 10. J Emerg Med. 2017. PMID: 27955984
Cited by
-
Early diagnosis of Gitelman syndrome in a young child: A case report.World J Clin Cases. 2022 Mar 26;10(9):2844-2850. doi: 10.12998/wjcc.v10.i9.2844. World J Clin Cases. 2022. PMID: 35434103 Free PMC article.
-
An early onset Gitelman syndrome presenting in a boy with failure to thrive with recurrent hypokalemia and hypomagnesemia: a case report.Pan Afr Med J. 2024 Oct 29;49:59. doi: 10.11604/pamj.2024.49.59.45186. eCollection 2024. Pan Afr Med J. 2024. PMID: 39911369 Free PMC article.
-
Normotensive hypokalemic primary hyperaldosteronism mimicking clinical features of anorexia nervosa in a young patient: A case report.Medicine (Baltimore). 2020 Jul 17;99(29):e20826. doi: 10.1097/MD.0000000000020826. Medicine (Baltimore). 2020. PMID: 32702825 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
