

Testicular histopathology, semen analysis and FSH, predictive value of sperm retrieval: supportive counseling in case of reoperation after testicular sperm extraction (TESE)
- PMID: 29973189
- PMCID: PMC6032772
- DOI: 10.1186/s12894-018-0379-7
Testicular histopathology, semen analysis and FSH, predictive value of sperm retrieval: supportive counseling in case of reoperation after testicular sperm extraction (TESE)
Abstract
Background: To provide indicators for the likelihood of sperm retrieval in patients undergoing testicular sperm extraction is a major issue in the management of male infertility by TESE. The aim of our study was to determine the impact of different parameters, including testicular histopathology, on sperm retrieval in case of reoperation in patients undergoing testicular sperm extraction.
Methods: We retrospectively analyzed 486 patients who underwent sperm extraction for intracytoplasmic sperm injection and testicular biopsy. Histology was classified into: normal spermatogenesis; hypospermatogenesis (reduction in the number of normal spermatogenetic cells); maturation arrest (absence of the later stages of spermatogenesis); and Sertoli cell only (absence of germ cells). Semen analysis and serum FSH, LH and testosterone were measured.
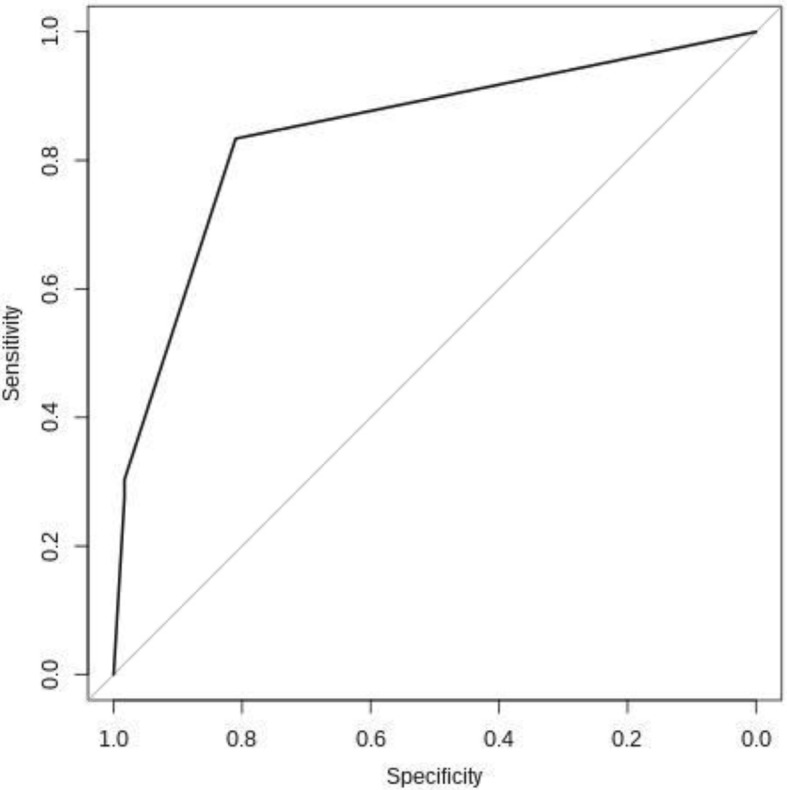
Results: Four hundred thirty patients had non obstructive azoospermia, 53 severe oligozoospermia and 3 necrozoospermia. There were 307 (63%) successful sperm retrieval. Higher testicular volume, lower levels of FSH, and better histological features were predictive for sperm retrieval. The same parameters and younger age were predictive factors for shorter time for sperm recovery. After multivariable analysis, younger age, better semen parameters, better histological features and lower values of FSH remained predictive for shorter time for sperm retrieval while better semen and histology remained predictive factors for successful sperm retrieval. The predictive capacity of a score obtained by summing the points assigned for selected predictors (1 point for Sertoli cell only, 0.33 points for azoospermia, 0.004 points for each FSH mIU/ml) gave an area under the ROC curve of 0.843.
Conclusions: This model can help the practitioner with counseling infertile men by reliably predicting the chance of obtaining spermatozoa with testicular sperm extraction when a repeat attempt is planned.
Keywords: FSH; Semen; Sperm retrieval; Testicular biopsy; Testicular sperm extraction (TESE).
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of the European Hospital, Rome, Italy and conducted in compliance with the principles of the Declaration of Helsinki. The patients included have signed written informed consent to publication of their case details and acknowledged that the results of this study did not affect the subsequent clinical course.
Consent for publication
The written informed consent for publication of details including the statistics of clinical, biochemistry, pathological, and radiological informations, was obtained from all the patients included in this study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia.BJU Int. 2013 Mar;111(3):492-9. doi: 10.1111/j.1464-410X.2012.11203.x. Epub 2012 May 15. BJU Int. 2013. PMID: 22583840
-
Successful testicular sperm extraction (TESE) in spite of high serum follicle stimulating hormone and azoospermia: correlation between testicular morphology, TESE results, semen analysis and serum hormone values in 103 infertile men.Hum Reprod. 1998 May;13(5):1230-4. doi: 10.1093/humrep/13.5.1230. Hum Reprod. 1998. PMID: 9647552
-
Testicular histology may predict the successful sperm retrieval in patients with non-obstructive azoospermia undergoing conventional TESE: a diagnostic accuracy study.J Assist Reprod Genet. 2017 Jan;34(1):149-154. doi: 10.1007/s10815-016-0812-3. Epub 2016 Sep 21. J Assist Reprod Genet. 2017. PMID: 27655389 Free PMC article.
-
[Predictive factors of testicular sperm extraction in men with non-obstructive azoospermia].Zhonghua Nan Ke Xue. 2016 May;22(5):462-6. Zhonghua Nan Ke Xue. 2016. PMID: 27416674 Review. Chinese.
-
Sperm retrieval for intra-cytoplasmic sperm injection in non-obstructive azoospermia.Minerva Urol Nefrol. 2005 Jun;57(2):99-107. Minerva Urol Nefrol. 2005. PMID: 15951734 Review.
Cited by
-
The infertile individual analysis based on whole-exome sequencing in chinese multi-ethnic groups.Genes Genomics. 2023 Apr;45(4):531-542. doi: 10.1007/s13258-022-01307-z. Epub 2022 Sep 17. Genes Genomics. 2023. PMID: 36115009
-
Testicular Sperm Extraction and Intracytoplasmic Sperm Injection in Management of Obstructive Azoospermia: A Two-Year Multicenter Review in Ghana.J Reprod Infertil. 2022 Oct-Dec;23(4):264-270. doi: 10.18502/jri.v23i4.10811. J Reprod Infertil. 2022. PMID: 36452196 Free PMC article.
-
Predictors of Successful Testicular Sperm Extraction: A New Era for Men with Non-Obstructive Azoospermia.Biomedicines. 2024 Nov 25;12(12):2679. doi: 10.3390/biomedicines12122679. Biomedicines. 2024. PMID: 39767586 Free PMC article. Review.
-
The Predictive Value of Serum Follicle-stimulating Hormone Level and Testicular Volume on the Outcome of Spermatozoa Retrieval from Testes in Men with Non-obstructive Azoospermia - A Retrospective Cohort Study.J Hum Reprod Sci. 2025 Jan-Mar;18(1):38-44. doi: 10.4103/jhrs.jhrs_9_25. Epub 2025 Mar 29. J Hum Reprod Sci. 2025. PMID: 40342883 Free PMC article.
-
Testicular ultrasound inhomogeneity is an informative parameter for fertility evaluation.Asian J Androl. 2020 May-Jun;22(3):302-308. doi: 10.4103/aja.aja_67_19. Asian J Androl. 2020. PMID: 31274478 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
