

Long term impact of CTLA4 blockade immunotherapy on regulatory and effector immune responses in patients with melanoma
- PMID: 29973204
- PMCID: PMC6033230
- DOI: 10.1186/s12967-018-1563-y
Long term impact of CTLA4 blockade immunotherapy on regulatory and effector immune responses in patients with melanoma
Abstract
Background: We previously reported early on-treatment significant modulation in circulating regulatory T cell (Treg), myeloid derived suppressor cells (MDSC) and antigen-specific type I CD4+ and CD8+ T cells that correlated with clinical outcome in regionally advanced melanoma patients treated with neoadjuvant ipilimumab. Here, we investigated the long term immunologic impact of CTLA4 blockade.
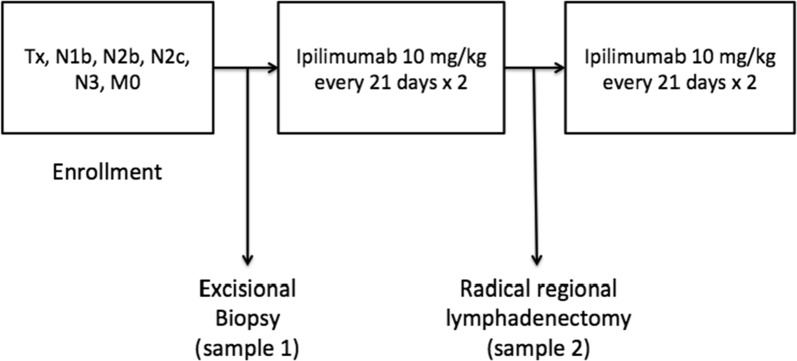
Methods: Patients were treated with ipilimumab given at 10 mg/kg IV every 3 weeks for 2 doses bracketing surgery. Blood specimens were collected at baseline and during treatment for up to 9 months. We tested immune responses at 3, 6, and 9 months utilizing multicolor flow cytometry. We compared frequencies of circulating Treg and MDSC on-study to baseline levels, as well as frequencies of CD4+ and CD8+ T cells specific to shared tumor-associated antigens (Gp-100, MART-1, NY-ESO-1).
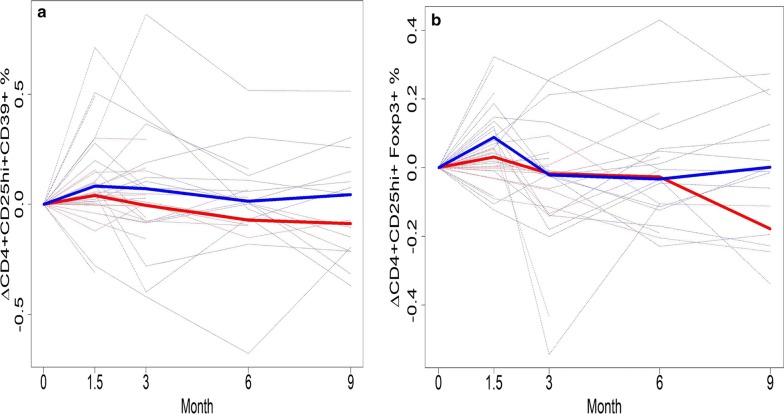
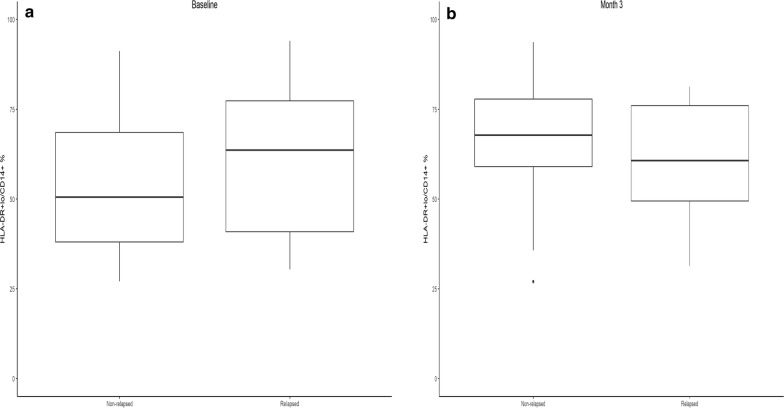
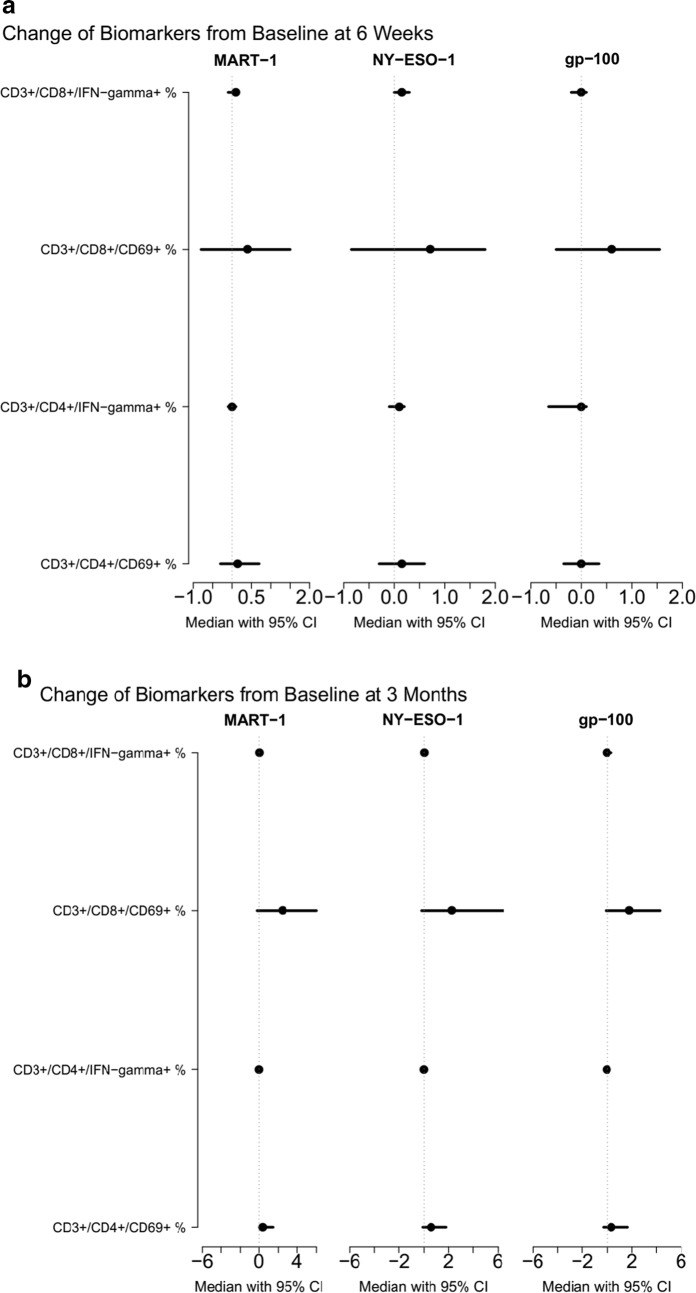
Results: Levels of Treg significantly increased when measured at 6 weeks following ipilimumab but returned to baseline by 3 months, with no significant difference in Treg levels between relapsed and relapse-free groups at 3, 6 or 9 months. However, lower baseline levels of circulating Treg (CD4+CD25hi+CD39+) were significantly associated with better relapse free survival (RFS) (p = 0.04). Levels of circulating monocytic HLA-DR+/loCD14+ MDSC were lower at baseline in the relapse-free group and further decreased at 6 weeks, though the differences did not reach statistical significance including measurements at 3, 6 or 9 months. We detected evidence of type I (interferon-γ producing), activated (CD69+) CD4+ and CD8+ antigen-specific T cell immunity against cancer-testis (NY-ESO-1) as well as melanocytic lineage (MART-1, gp100) antigens in the absence of therapeutic vaccination. These responses were significantly boosted at 6 weeks and persisted at 3, 6 and 9 months following the initiation of ipilimumab.
Conclusions: Lower Treg levels at baseline are significantly associated with RFS and increased Treg frequency after CTLA4 blockade was only transient. Lower MDSC was also associated with RFS and MDSC levels were further decreased after ipilimumab. Tumor specific effector immune responses are boosted with CTLA4 blockade and tend to be durable. Trial registration ClinicalTrials.gov Identifier: NCT00972933.
Keywords: CTLA4; Ipilimumab; MDSC; Melanoma; Regulatory T cells; Tumor antigens.
Figures


References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
