

mHealth intervention to improve the continuum of maternal and perinatal care in rural Guatemala: a pragmatic, randomized controlled feasibility trial
- PMID: 29973229
- PMCID: PMC6033207
- DOI: 10.1186/s12978-018-0554-z
mHealth intervention to improve the continuum of maternal and perinatal care in rural Guatemala: a pragmatic, randomized controlled feasibility trial
Abstract
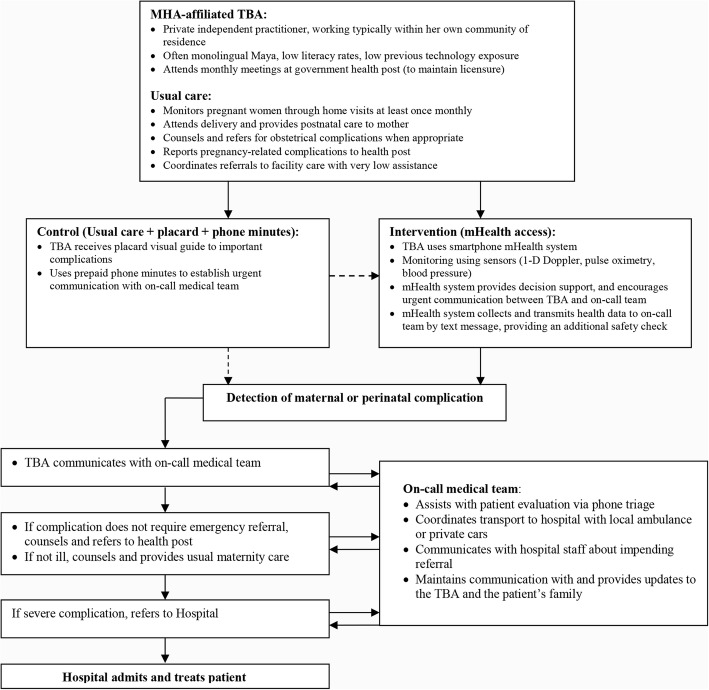
Background/objective: Guatemala's indigenous Maya population has one of the highest perinatal and maternal mortality rates in Latin America. In this population most births are delivered at home by traditional birth attendants (TBAs), who have limited support and linkages to public hospitals. The goal of this study was to characterize the detection of maternal and perinatal complications and rates of facility-level referral by TBAs, and to evaluate the impact of a mHealth decision support system on these rates.
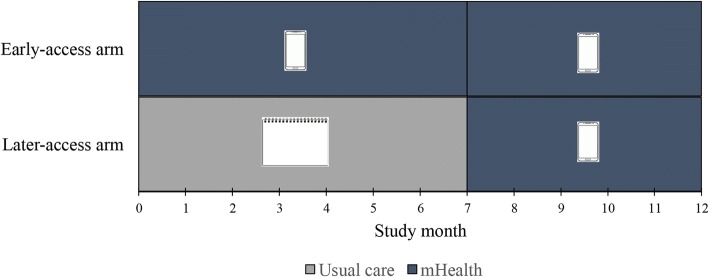
Methods: A pragmatic one-year feasibility trial of an mHealth decisions support system was conducted in rural Maya communities in collaboration with TBAs. TBAs were individually randomized in an unblinded fashion to either early-access or later-access to the mHealth system. TBAs in the early-access arm used the mHealth system throughout the study. TBAs in the later-access arm provided usual care until crossing over uni-directionally to the mHealth system at the study midpoint. The primary study outcome was the monthly rate of referral to facility-level care, adjusted for birth volume.
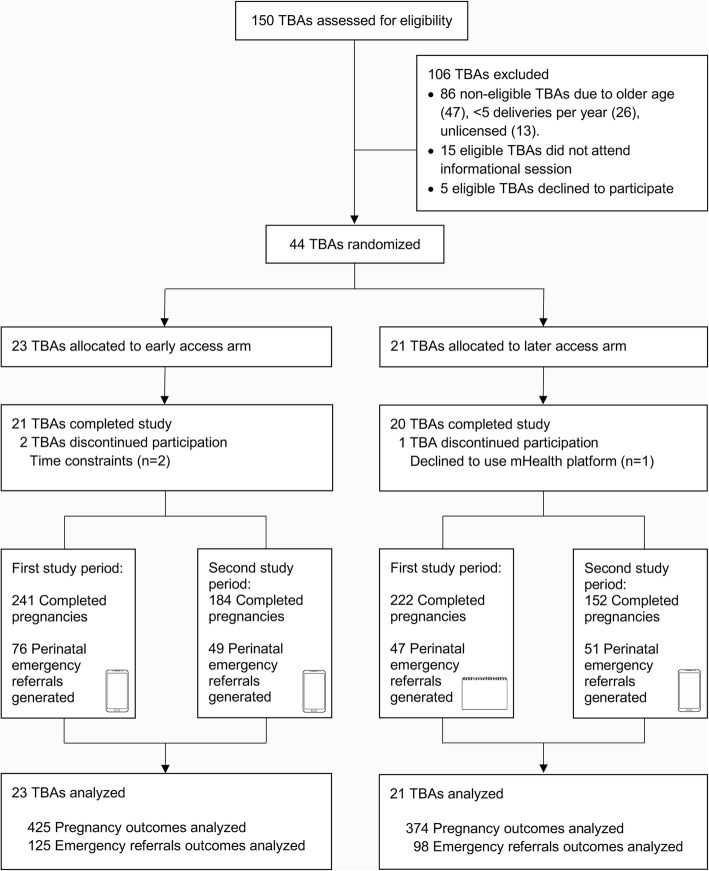
Results: Forty-four TBAs were randomized, 23 to the early-access arm and 21 to the later-access arm. Outcomes were analyzed for 799 pregnancies (early-access 425, later-access 374). Monthly referral rates to facility-level care were significantly higher among the early-access arm (median 33 referrals per 100 births, IQR 22-58) compared to the later-access arm (median 20 per 100, IQR 0-30) (p = 0.03). At the study midpoint, the later-access arm began using the mHealth platform and its referral rates increased (median 34 referrals per 100 births, IQR 5-50) with no significant difference from the early-access arm (p = 0.58). Rates of complications were similar in both arms, except for hypertensive disorders of pregnancy, which were significantly higher among TBAs in the early-access arm (RR 3.3, 95% CI 1.10-9.86).
Conclusions: Referral rates were higher when TBAs had access to the mHealth platform. The introduction of mHealth supportive technologies for TBAs is feasible and can improve detection of complications and timely referral to facility-care within challenging healthcare delivery contexts.
Trial registration: Clinicaltrials.gov NCT02348840 .
Keywords: Barriers to care; Guatemala; Indigenous; Lay midwives; Perinatal monitoring; Referral system; Resource-constrained healthcare; Traditional birth attendants; mHealth.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Review Boards of Maya Health Alliance (Protocol number WK-2015-001) and Emory University (Protocol number IRB00076231). Written informed consent to participate was obtained from traditional birth attendants and subjects involved in the study.
Consent for publication
Not applicable.
Competing interests
BM, ECI, MJ, and PR are current staff members at Maya Health Alliance, the partnering healthcare organization for this study in Guatemala; the authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- United Nations. Sustainable Development Goals. http://www.un.org/sustainabledevelopment/health/ (2015). Accessed 10 Oct 2017.
-
- World Health Organization . Fact sheet #348. Geneva: World Health Organization; 2015. Maternal mortality.
-
- World Health Organization . Maternal and perinatal health. Geneva: World Health Organization; 2016.
-
- The World Bank. Indicator: Maternal mortality ratio.http://data.worldbank.org/indicator/SH.STA.MMRT (2015). Accessed 10 Oct 2017.
-
- The World Bank. Indicator: Mortality rate, under-5 (per 1,000 live births). http://data.worldbank.org/indicator/SH.DYN.MORT (2016). Accessed 11 Oct 2017.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
