

Risks and benefits of direct oral anticoagulants versus warfarin in a real world setting: cohort study in primary care
- PMID: 29973392
- PMCID: PMC6031213
- DOI: 10.1136/bmj.k2505
Risks and benefits of direct oral anticoagulants versus warfarin in a real world setting: cohort study in primary care
Erratum in
-
Risks and benefits of direct oral anticoagulants versus warfarin in a real world setting: cohort study in primary care.BMJ. 2018 Oct 18;363:k4413. doi: 10.1136/bmj.k4413. BMJ. 2018. PMID: 30337336 No abstract available.
Abstract
Objective: To investigate the associations between direct oral anticoagulants (DOACs) and risks of bleeding, ischaemic stroke, venous thromboembolism, and all cause mortality compared with warfarin.
Design: Prospective open cohort study.
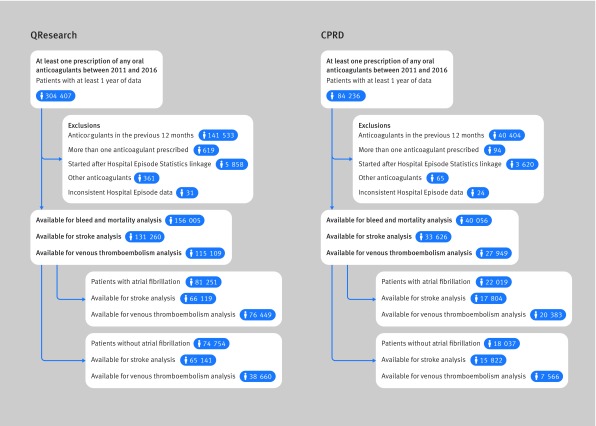
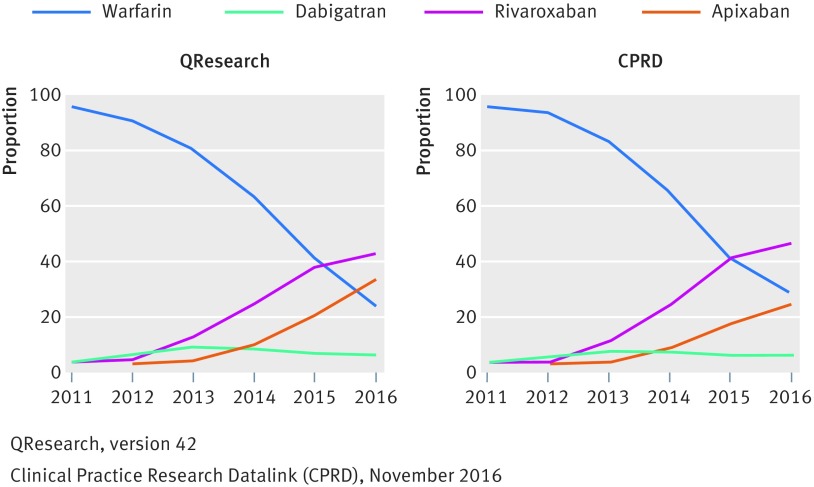
Setting: UK general practices contributing to QResearch or Clinical Practice Research Datalink.
Participants: 132 231 warfarin, 7744 dabigatran, 37 863 rivaroxaban, and 18 223 apixaban users without anticoagulant prescriptions for 12 months before study entry, subgrouped into 103 270 patients with atrial fibrillation and 92 791 without atrial fibrillation between 2011 and 2016.
Main outcome measures: Major bleeding leading to hospital admission or death. Specific sites of bleeding and all cause mortality were also studied.
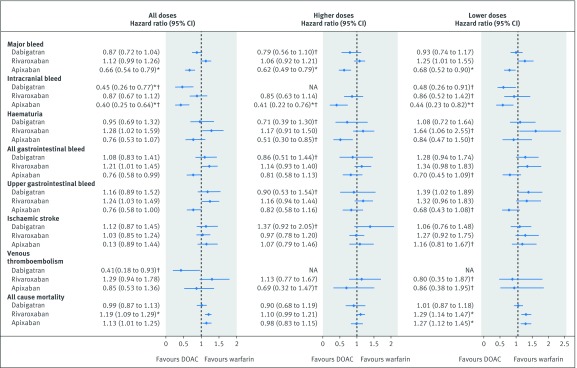
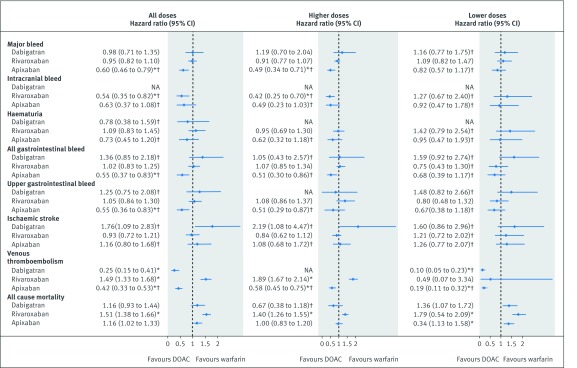
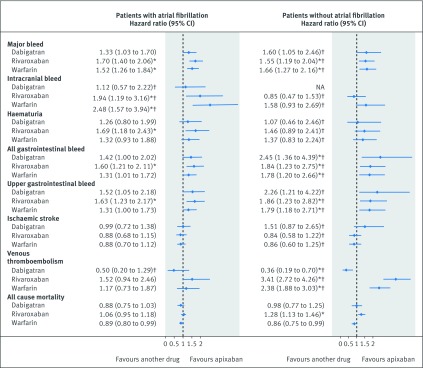
Results: In patients with atrial fibrillation, compared with warfarin, apixaban was associated with a decreased risk of major bleeding (adjusted hazard ratio 0.66, 95% confidence interval 0.54 to 0.79) and intracranial bleeding (0.40, 0.25 to 0.64); dabigatran was associated with a decreased risk of intracranial bleeding (0.45, 0.26 to 0.77). An increased risk of all cause mortality was observed in patients taking rivaroxaban (1.19, 1.09 to 1.29) or on lower doses of apixaban (1.27, 1.12 to 1.45). In patients without atrial fibrillation, compared with warfarin, apixaban was associated with a decreased risk of major bleeding (0.60, 0.46 to 0.79), any gastrointestinal bleeding (0.55, 0.37 to 0.83), and upper gastrointestinal bleeding (0.55, 0.36 to 0.83); rivaroxaban was associated with a decreased risk of intracranial bleeding (0.54, 0.35 to 0.82). Increased risk of all cause mortality was observed in patients taking rivaroxaban (1.51, 1.38 to 1.66) and those on lower doses of apixaban (1.34, 1.13 to 1.58).
Conclusions: Overall, apixaban was found to be the safest drug, with reduced risks of major, intracranial, and gastrointestinal bleeding compared with warfarin. Rivaroxaban and low dose apixaban were, however, associated with increased risks of all cause mortality compared with warfarin.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no support from any additional organisation for the submitted work. JHC is professor of clinical epidemiology at the University of Nottingham and unpaid director of QResearch, a not-for-profit organisation which is a joint partnership between the University of Nottingham and EMIS (commercial IT supplier for 60% of general practices in the UK). JHC is also a paid director of ClinRisk Limited, which produces open and closed source software to ensure the reliable and updatable implementation of clinical risk algorithms (including QRISK2) within clinical computer systems to help improve patient care. There have been no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- National Institute for Clinical Excellence. Venous thromboembolism in adults admitted to hospital: reducing the risk. In: NICE clinical guideline 92, ed. London: NICE, 2010 https://www.nice.org.uk/guidance/ng89
-
- Mant J, Hobbs FDR, Fletcher K, et al. BAFTA investigators. Midland Research Practices Network (MidReC) Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 2007;370:493-503. 10.1016/S0140-6736(07)61233-1 - DOI - PubMed
-
- National Institute for Clinical Excellence. Anticoagulants, including non-vitamin K antagonist oral anticoagulants (NOACs). Key theraputic topic 2016;KTT16 https://www.nice.org.uk/advice/ktt16/chapter/Options-for-local-implement...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical