

doi: 10.1161/JAHA.118.008587.
Definition and Management of Segmental Pulmonary Hypertension
Affiliations
- PMID: 29973393
- PMCID: PMC6064837
- DOI: 10.1161/JAHA.118.008587
Item in Clipboard
Definition and Management of Segmental Pulmonary Hypertension
J Am Heart Assoc.
.
No abstract available
Keywords: congenital heart disease; pulmonary atresia; pulmonary hypertension; segmental pulmonary hypertension; truncus arteriosus.
Figures
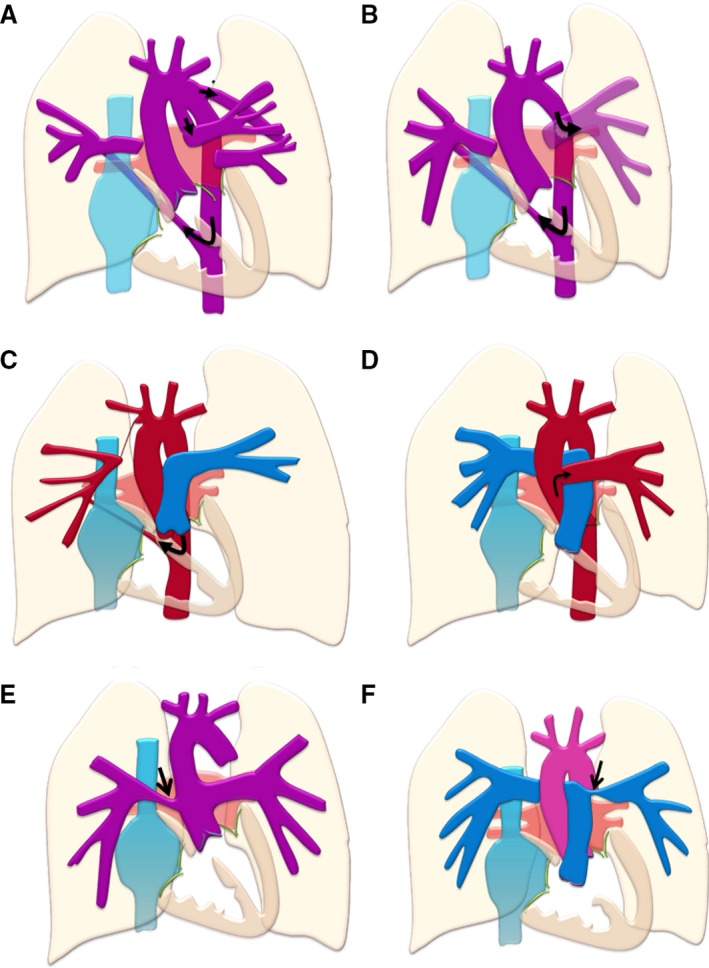
Schematic examples of segmental pulmonary hypertension. In (A), complex pulmonary atresia, with nonconfluent pulmonary arteries supplied by a patent ductus arteriosus and major aortopulmonary collateral arteries (MAPCA s) from the descending aorta (arrows), is shown. In (B), the left pulmonary artery is supplied by a Potts shunt and the right by a MAPCA from the descending aorta (arrows). Potts (descending aorta to left pulmonary artery) and Waterston (ascending aorta to right pulmonary artery) shunts are difficult to size and are therefore more likely to cause pressure and volume overload of the lung segments supplied, over time leading to the development of segmental pulmonary hypertension. In (C), unilateral absence of right pulmonary artery or isolated right pulmonary artery of ductal origin. There is a small outpouching of the innominate artery and a ductal remnant to the isolated pulmonary artery. The latter is supplied by a large MAPCA from the descending aorta (arrow), which may cause pulmonary hypertension (PH ) to develop in the right lung. Pulmonary hypertension may also develop in the left lung only. In (D), hemitruncus arteriosus, with the left pulmonary artery arising from the hemitruncus (arrow) and the right from the main pulmonary artery in direct communication with the right ventricle. Only the left lung is hypertensive. In (E), common arterial trunk with stenosis of the origin of the right pulmonary artery (arrow) is shown. In this case, only the left lung is hypertensive. In (F), there is a large ventricular septal defect (VSD ), and stenosis of the origin of the left pulmonary artery (arrow). In this condition, shunting through the nonrestrictive VSD is likely to cause distal PH and pulmonary vascular disease in the right, but not the left lung. Right‐to‐left shunting may be caused by right heart remodeling as a result of the combination of proximal left branch PA stenosis and distal right pulmonary vascular disease (PH ).
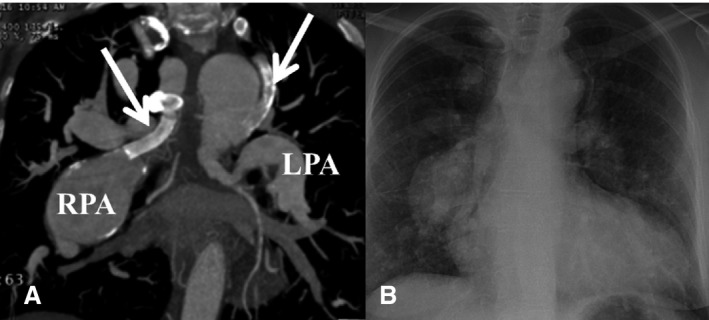
Tetralogy of Fallot with complex pulmonary atresia and previous bilateral Blalock Taussig shunts (A, arrows). The right pulmonary artery (RPA ) is hypertensive and severely dilated, while the left pulmonary artery (LPA ) is supplied by a relatively small collateral and is of normal caliber. This patient has segmental pulmonary hypertension, with pulmonary hypertension of various severities in different segments of the lung (eg, right mid and lower), while other segments are normotensive and may be hypoperfused. In (B), chest radiograph of the same patient shows a boot‐shaped heart with inhomogeneous pulmonary vascular markings.
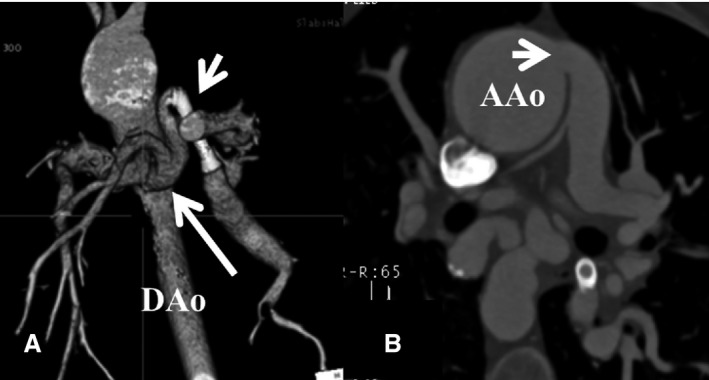
Computed tomography scan of a patient with tetralogy of Fallot and complex pulmonary atresia. In (A), major aortopulmonary collateral arteries (MAPCA s, arrow) arising from the descending aorta (DA o), some of which are large and may cause pulmonary hypertension in the areas supplied, while others are narrow and have required stenting to ensure adequate perfusion in the respective lung segments. In (B), a large MAPCA (arrow) arising from the ascending aorta (AA o) and supplying a hypertensive lung segment is seen. Numerous other MAPCA s are seen within the mediastinum. Ascending aortic dilation is apparent.
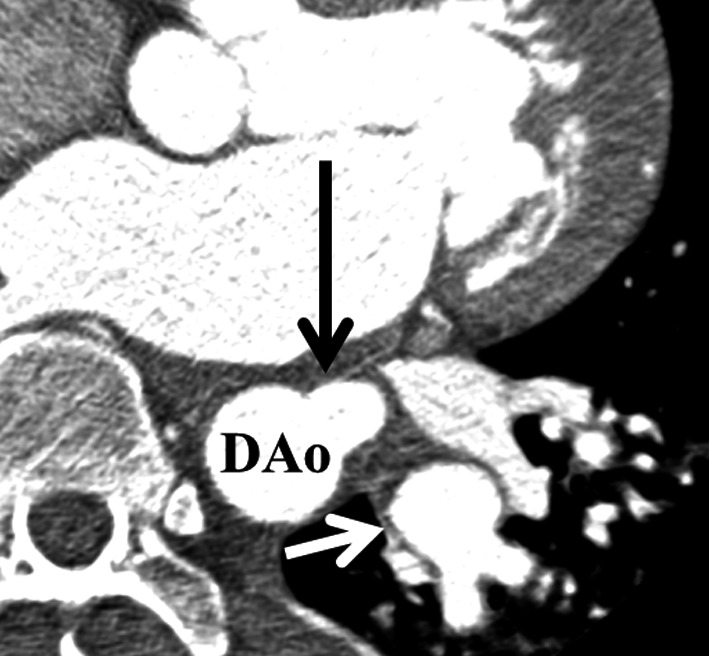
Anomalous origin of the left lower pulmonary artery (black arrow) from the descending aorta (DA o). The distal branches of the left lower pulmonary artery (white arrow) are dilated. There is segmental pulmonary hypertension limited in the left lower lung lobe.
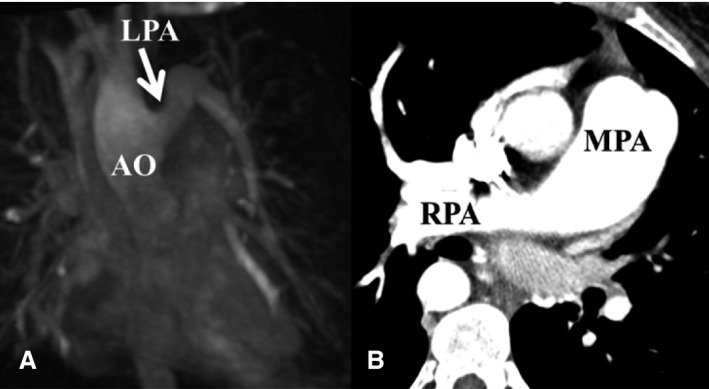
Hemitruncus arteriosus. In (A), the left pulmonary artery (LPA ) is seen on cardiac magnetic resonance arising from the ascending aorta (AO ). In (B), the right pulmonary artery (RPA ) arises from the main pulmonary artery (MPA ). In this situation, the left lung is hypertensive while the right is not, in the absence of associated CHD (eg, large VSD or PDA to the RPA ). CHD indicates congenital heart disease; PDA , patent ductus arteriosus; VSD , ventricular septal defect.
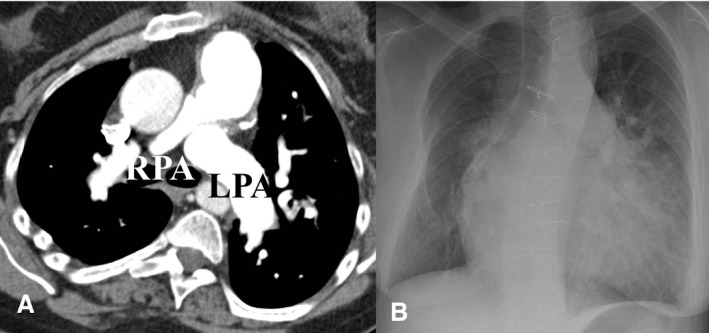
Tetralogy of Fallot and complex pulmonary atresia after conduit repair and closure of the ventricular septal defect, but with a significant residual shunt. In (A), there is significant pulmonary hypertension in the left lung with a dilated left pulmonary artery (LPA ), while the right lung is “protected” by a stenosed right pulmonary artery (RPA ). In (B), severe cardiomegaly with prominent pulmonary vascular marking in the hypertensive left lung are seen, but not in the right lung. Kyphoscoliosis, common in this group of patients, is also apparent and can independently impair pulmonary gas exchange and predispose towards pulmonary vascular remodeling in severe cases.
References
-
- Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, Gomez Sanchez MA, Krishna Kumar R, Landzberg M, Machado RF, Olschewski H, Robbins IM, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D34–D41. - PubMed
-
- Galiè N, Humbert M, Vachiery J‐L, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, Aboyans V, Vaz Carneiro A, Achenbach S, Agewall S, Allanore Y, Asteggiano R, Paolo Badano L, Albert Barberà J, Bouvaist H, Bueno H, Byrne RA, Carerj S, Castro G, Erol Ç, Falk V, Funck‐Brentano C, Gorenflo M, Granton J, Iung B, Kiely DG, Kirchhof P, Kjellstrom B, Landmesser U, Lekakis J, Lionis C, Lip GYH, Orfanos SE, Park MH, Piepoli MF, Ponikowski P, Revel M‐P, Rigau D, Rosenkranz S, Völler H, Luis Zamorano J. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37:67–119. - PubMed
-
- Schuuring MJ, Bouma BJ, Cordina R, Gatzoulis MA, Budts W, Mullen MP, Vis JC, Celermajer D, Mulder BJM. Treatment of segmental pulmonary artery hypertension in adults with congenital heart disease. Int J Cardiol. 2013;164:106–110. - PubMed
-
- Tchervenkov CI, Roy N. Congenital Heart Surgery Nomenclature and Database Project: pulmonary atresia—ventricular septal defect. Ann Thorac Surg. 2000;69:S97–S105. - PubMed
-
- Barbero‐Marcial M. Classification of pulmonary atresia with ventricular septal defect. Ann Thorac Surg. 2001;72:316–317. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
