

Longitudinal Changes of Caudate-Based Resting State Functional Connectivity in Mild Traumatic Brain Injury
- PMID: 29973909
- PMCID: PMC6020789
- DOI: 10.3389/fneur.2018.00467
Longitudinal Changes of Caudate-Based Resting State Functional Connectivity in Mild Traumatic Brain Injury
Abstract
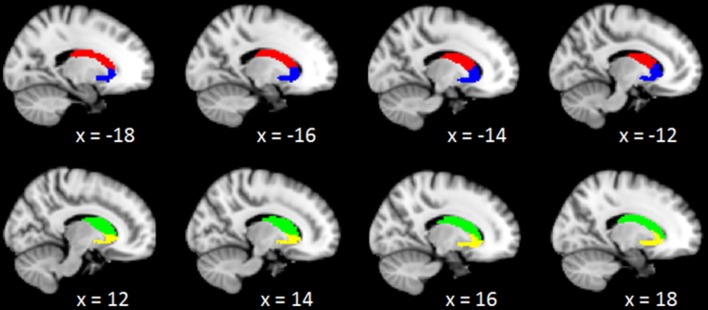
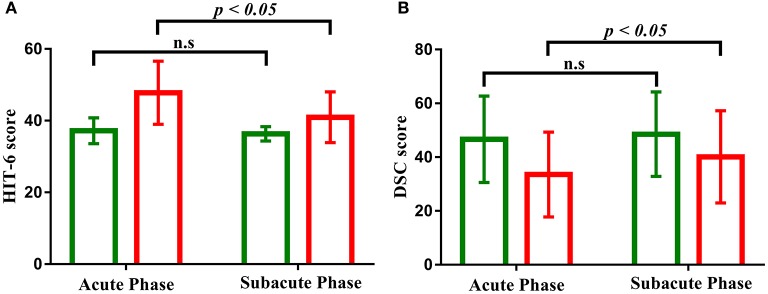
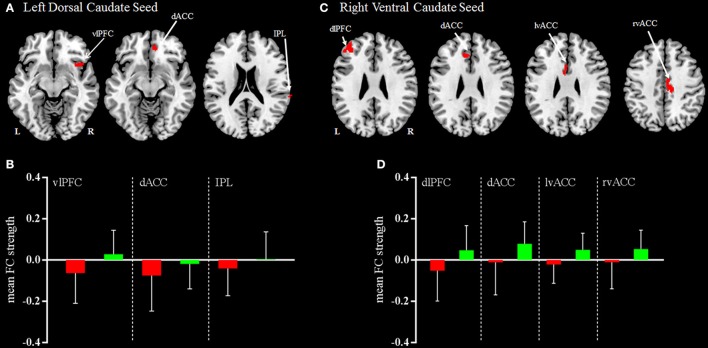
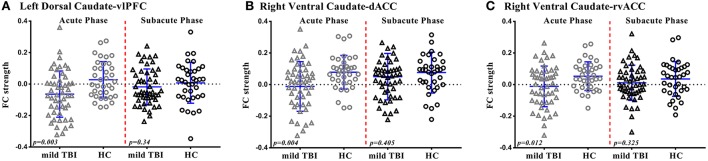
Mild traumatic brain injury (mild TBI) is associated with dysfunctional brain network and accumulating evidence is pointing to the caudate as a vulnerable hub region. However, little is known about the longitudinal changes in the caudate-based resting-state functional connectivity following mild TBI. In the current study, 50 patients with mild TBI received resting-state functional magnetic resonance imaging as well as neuropsychological assessments within 7 days post-injury (acute phase) and 1 month later (subacute phase). Thirty-six age- and gender- matched healthy controls underwent the same protocol. The caudate was segmented into the dorsal and ventral sub-regions based on their related functionally distinct neural circuits and separate functional connectivity was investigated. Results indicated that patients with mild TBI at acute phase exhibited reduced left dorsal caudate-based functional connectivity with ventral lateral prefrontal cortex, dorsal anterior cingulate cortex, and inferior parietal lobule, which mainly distributed in the cognitive control network, and reduced right ventral caudate-based functional connectivity with the dorsal lateral prefrontal cortex, dorsal anterior cingulate cortex (dACC), and bilateral ventral anterior cingulate cortex (vACC), which mainly distributed in the executive network and emotional processing network. Furthermore, patients with mild TBI presented the reduced functional connectivity between the left dorsal caudate and the ventral lateral prefrontal cortex (vlPFC) compared with healthy controls at acute phase while this difference became no significance and return to the normal level following 1 month post-injury subacute phase. Similarly, the functional connectivity between the right ventral caudate and anterior cingulate cortex (both dorsal and ventral part) showed the reduced strength in patients compared with healthy controls only at the acute phase but presented no significant difference at subacute phase following mild TBI. Along the same line, patients with mild TBI presented the impaired performance on the information processing speed and more complaints on the pain impact index at acute phase compared with healthy controls but showed no significant difference at the follow-up 1 month post-injury subacute phase. The longitudinal changes of caudate-based dysfunction connectivity could serve as a neuroimaging biomarker following patients with mild TBI, with the evidence that the abnormal caudate-based functional connectivity at acute phase have returned to the normal level accompanying with the recovery of the neuropsychological syndromes following patients with mild TBI at subacute phase.
Keywords: a neuroimaging biomarker; caudate; dysfunction; longitudinal changes; mild traumatic brain injury.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources