

Early medical abortion with self-administered low-dose mifepristone in combination with misoprostol
- PMID: 29974571
- PMCID: PMC6175481
- DOI: 10.1111/jog.13716
Early medical abortion with self-administered low-dose mifepristone in combination with misoprostol
Abstract
Aim: The aim of the present study was to investigate the safety and efficacy of low-dose mifepristone combined with self-administered misoprostol for termination of early pregnancy.
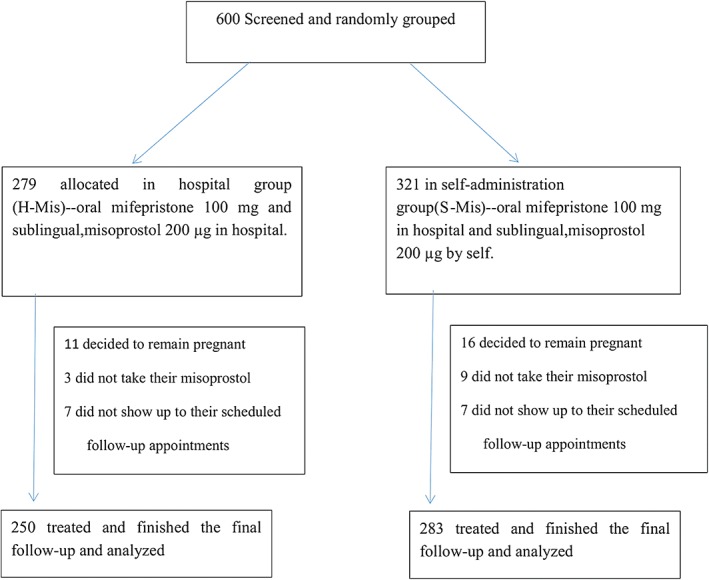
Methods: A total of 533 women seeking medical abortion in early pregnancy (≤49 days since the last menstrual period) were divided randomly into hospital- (H-Mis, 250) and self- (S-Mis, 283) administered misoprostol groups. Women in two groups took 100 mg of oral mifepristone in hospital followed by 200 μg of sublingual misoprostol 24 h later in hospital or home. The primary outcome parameter was complete abortion without surgical intervention. Secondary outcomes were uterine bleeding, return of regular menses, side effects and patient acceptability.
Results: High rates of complete abortion were observed for both the H-Mis group (243/250; 94.8%) and the S-Mis group (266/283; 94.0%). No significant differences in outcomes (complete abortion/failure rates) or side effects were observed between the two groups. General satisfaction rates were similar for the two groups (H-Mis, 231/250, 92.4%; S-Mis, 263/283, 92.9%; P > 0.05). Higher convenience of administration (H-Mis, 211/250, 84.4%; S-Mis, 270/283, 95.4%; P < 0.05) and privacy protection (H-Mis, 214/250, 85.6%; S-Mis, 267/283, 94.3%; P < 0.05) satisfaction rates were obtained for the S-Mis group than for the H-Mis group.
Conclusion: Self-administered sublingual misoprostol is as safe and effective as hospital-administered misoprostol following low-dose mifepristone to terminate early pregnancy (≤49 days of amenorrhoea) with fewer side effects.
Keywords: early medical abortion; low-dose; mifepristone and misoprostol; self-administration.
© 2018 The Authors. Journal of Obstetrics and Gynaecology Research published by John Wiley & Sons Australia, Ltd on behalf of Japan Society of Obstetrics and Gynecology.
Figures
References
-
- Gardner DK, Kelley RL. Impact of the IVF laboratory environment on human preimplantation embryo phenotype. J Dev Orig Health Dis 2017; 8: 418–435. - PubMed
-
- Khurana NK, Niemann H. Energy metabolism in preimplantation bovine embryos derived in vitro or in vivo . Biol Reprod 2000; 62: 847–856. - PubMed
-
- Heikinheimo O, Leminen R, Suhonen S. Termination of early pregnancy using flexible, low‐dose mifepristone‐misoprostol regimens. Contraception 2007; 76: 456–460. - PubMed
-
- Anonymous . Lowering the doses of mifepristone and gameprost for early abortion: A randomised controlled trial World Health Organization Task Force on Post‐Ovulatory Methods for Fertility Regulation. BJOG 2001; 108: 738–742. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
