

Effectiveness of a multidisciplinary patient care bundle for reducing surgical-site infections
- PMID: 29974946
- PMCID: PMC6190910
- DOI: 10.1002/bjs.10896
Effectiveness of a multidisciplinary patient care bundle for reducing surgical-site infections
Abstract
Background: Surgical-site infection (SSI) is associated with significant healthcare costs. To reduce the high rate of SSI among patients undergoing colorectal surgery at a cancer centre, a comprehensive care bundle was implemented and its efficacy tested.
Methods: A pragmatic study involving three phases (baseline, implementation and sustainability) was conducted on patients treated consecutively between 2013 and 2016. The intervention included 13 components related to: bowel preparation; oral and intravenous antibiotic selection and administration; skin preparation, disinfection and hygiene; maintenance of normothermia during surgery; and use of clean instruments for closure. SSI risk was evaluated by means of a preoperative calculator, and effectiveness was assessed using interrupted time-series regression.
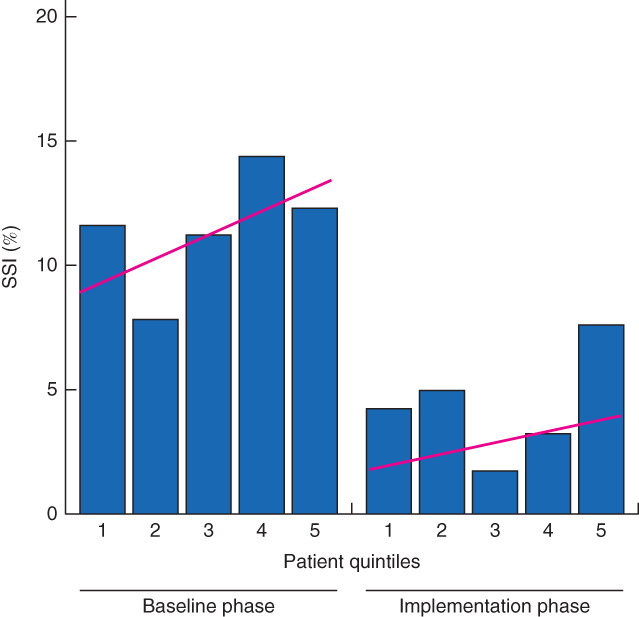
Results: In a population with a mean BMI of 30 kg/m2 , diabetes mellitus in 17·5 per cent, and smoking history in 49·3 per cent, SSI rates declined from 11·0 to 4·1 per cent following implementation of the intervention bundle (P = 0·001). The greatest reductions in SSI rates occurred in patients at intermediate or high risk of SSI: from 10·3 to 4·7 per cent (P = 0·006) and from 19 to 2 per cent (P < 0·001) respectively. Wound care modifications were very different in the implementation phase (43·2 versus 24·9 per cent baseline), including use of an overlying surface vacuum dressing (17·2 from 1·4 per cent baseline) or leaving wounds partially open (13·2 from 6·7 per cent baseline). As a result, the biggest difference was in wound-related rather than organ-space SSI. The median length of hospital stay decreased from 7 (i.q.r. 5-10) to 6 (5-9) days (P = 0·002). The greatest reduction in hospital stay was seen in patients at high risk of SSI: from 8 to 6 days (P < 0·001). SSI rates remained low (4·5 per cent) in the sustainability phase.
Conclusion: Meaningful reductions in SSI can be achieved by implementing a multidisciplinary care bundle at a hospital-wide level.
© 2018 BJS Society Ltd Published by John Wiley & Sons Ltd.
Figures

References
-
- Scott RD. The Direct Medical Costs of Healthcare Associated Infection in U.S. Hospitals and the Benefits of Prevention; 2009. www.cdc.gov/hai/pdfs/hai/Scott_CostPaper.pdf [accessed 30 January 2018].
-
- Anderson DJ, Kaye KS. Staphylococcal surgical site infections. Infect Dis Clin North Am 2009; 23: 53–72. - PubMed
-
- Artinyan A, Orcutt ST, Anaya DA, Richardson P, Chen GJ, Berger DH. Infectious postoperative complications decrease long-term survival in patients undergoing curative surgery for colorectal cancer: a study of 12 075 patients. Ann Surg 2015; 261: 497–505. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
