

Clinical application and technical considerations of T1 & T2(*) mapping in cardiac, liver, and renal imaging
- PMID: 29975154
- PMCID: PMC6319842
- DOI: 10.1259/bjr.20170825
Clinical application and technical considerations of T1 & T2(*) mapping in cardiac, liver, and renal imaging
Abstract
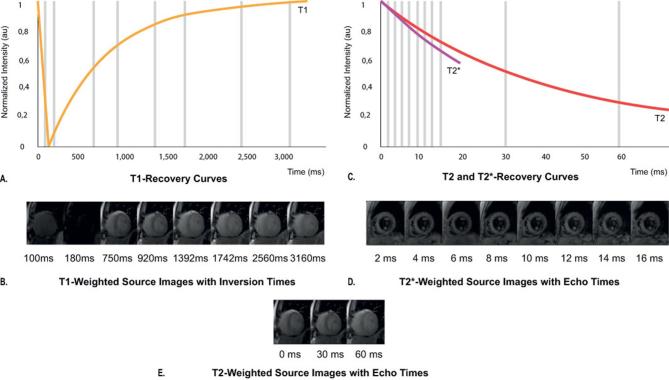
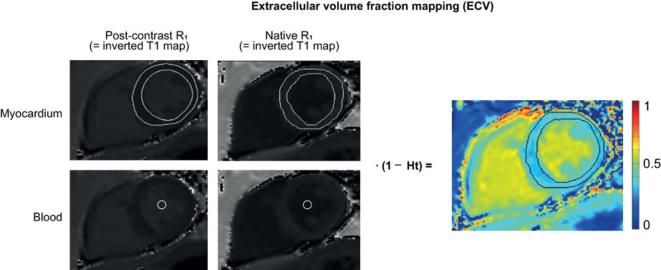
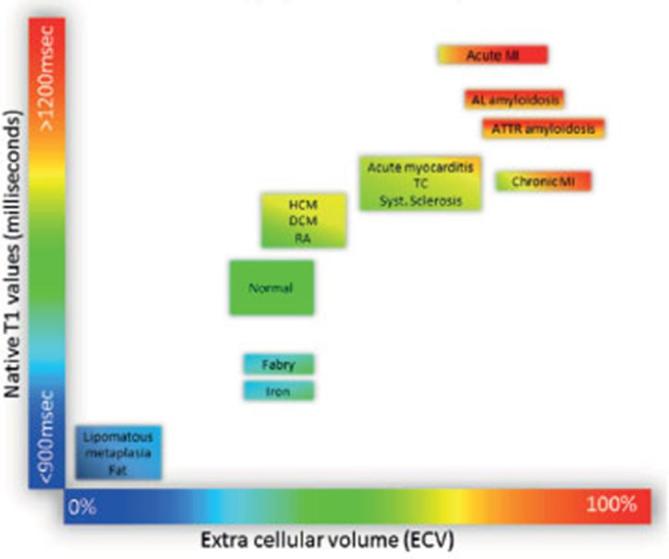
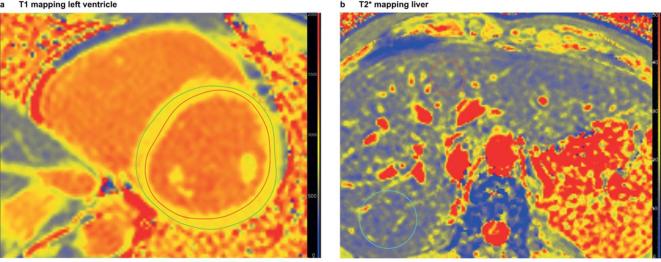
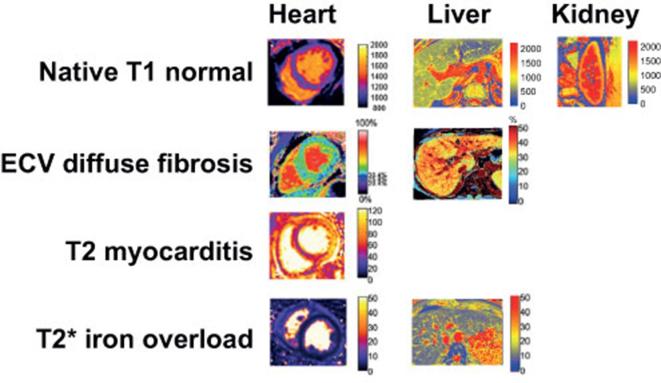
Pathological tissue alterations due to disease processes such as fibrosis, edema and infiltrative disease can be non-invasively visualized and quantified by MRI using T1 and T2 relaxation properties. Pixel-wise mapping of T1 and T2 image sequences enable direct quantification of T1, T2(*), and extracellular volume values of the target organ of interest. Tissue characterization based on T1 and T2(*) mapping is currently making the transition from a research tool to a clinical modality, as clinical usefulness has been established for several diseases such as myocarditis, amyloidosis, Anderson-Fabry and iron deposition. Other potential clinical applications besides the heart include, quantification of steatosis, cirrhosis, hepatic siderosis and renal fibrosis. Here, we provide an overview of potential clinical applications of T1 andT2(*) mapping for imaging of cardiac, liver and renal disease. Furthermore, we give an overview of important technical considerations necessary for clinical implementation of quantitative parametric imaging, involving data acquisition, data analysis, quality assessment, and interpretation. In order to achieve clinical implementation of these techniques, standardization of T1 and T2(*) mapping methodology and validation of impact on clinical decision making is needed.
Figures
References
-
- Scallan J, Huxley V, Korthuis R, Fluid C. Exchange: regulation, functions, and pathology. Integrated systems physiology: from molecule to function to disease. San Rafael, CA: The British Institute of Radiology.; 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
