

Red cell distribution width and red cell distribution width to total serum calcium ratio as major predictors of severity and mortality in acute pancreatitis
- PMID: 29976140
- PMCID: PMC6034316
- DOI: 10.1186/s12876-018-0834-7
Red cell distribution width and red cell distribution width to total serum calcium ratio as major predictors of severity and mortality in acute pancreatitis
Abstract
Background: Acute pancreatitis (AP) is associated with considerable morbidity and mortality. Current severity scores include multiple variables and some of them are only complete within 48 h of admission. Red cell distribution width (RDW) is a simple and routine parameter that seems to be related to inflammatory status. Our aims were to evaluate the diagnostic value of RDW in severity and mortality of AP comparing with other prognostic scoring systems.
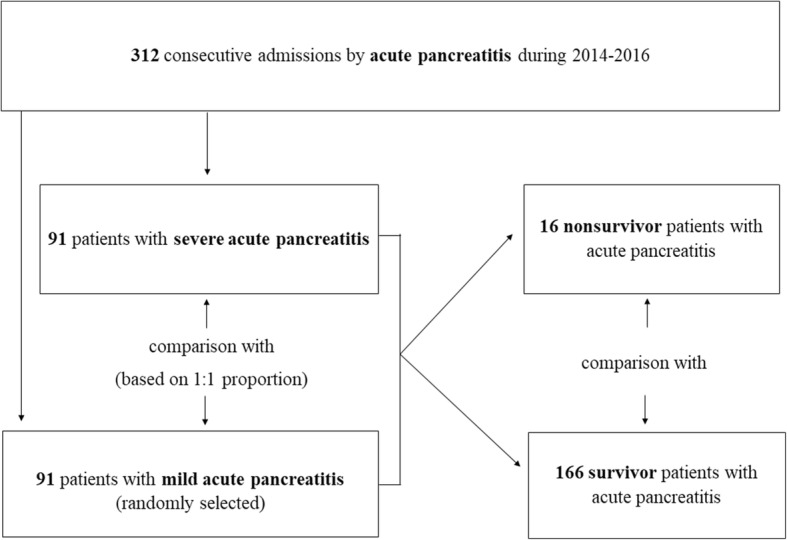
Methods: Retrospective case-control study of a total of 312 patients with AP admitted between 2014 and 2016. Patients with severe AP (cases) were compared with patients with mild AP (controls) in the 1:1 proportion. Additionally, a comparison between survivor and nonsurvivor AP patients was performed. Diagnosis and severity of AP were defined according to the revised Atlanta classification 2012. Variables evaluated included demographics, comorbidities, hospital stay, laboratorial parameters, arterial blood gas analysis, prognostic scores within 24 h of admission (Ranson, BISAP and Modified Marshall) and mortality.
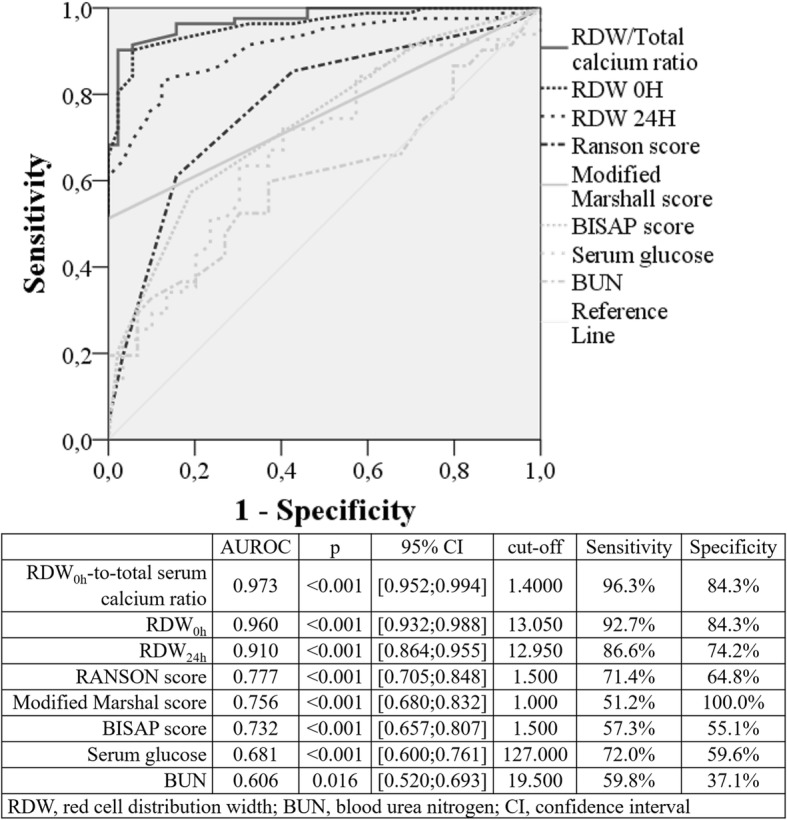
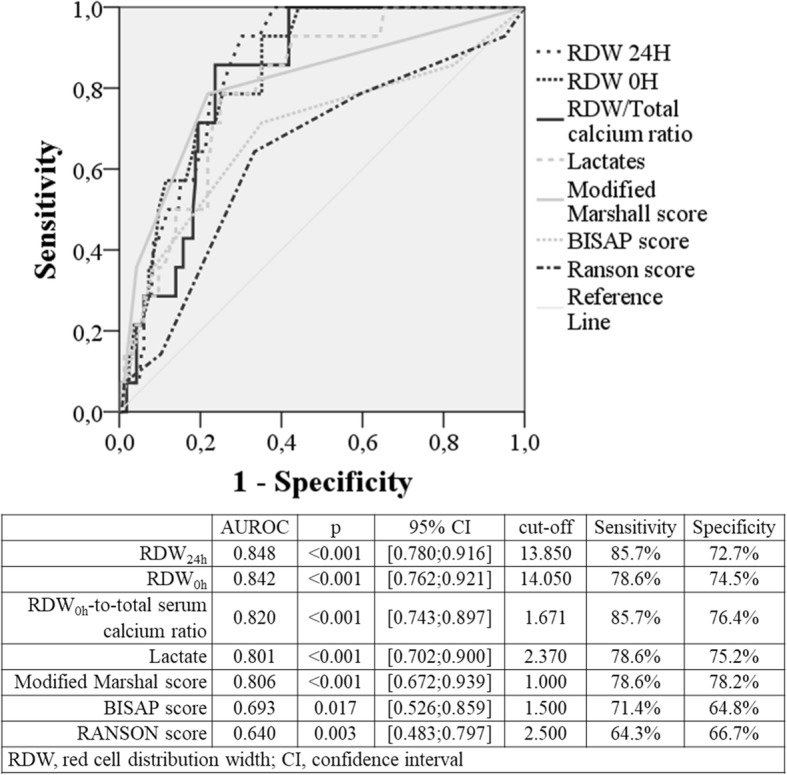
Results: Included 91 cases of severe AP, most males (58.2% vs 51.6%; p = 0.228) with mean age of 64.8 ± 16.3 years (vs 67.9 ± 13.7; p = 0.239). RDW0h was higher in patients with severe AP (14.6 ± 1.3 vs 12.7 ± 0.5; p < 0.001), as well as RDW0h-to-serum calcium ratio (1.8 ± 0.3 vs 1.3 ± 0.1; p < 0.001). After multivariate and ROC curve analysis, RDW0h (AUROC: 0.960; p < 0.001) and RDW0h-to-serum calcium ratio (AUROC: 0.973; p < 0.001) were the major predictors of severe AP for a cut-off value of 13.0 (S: 92.7%; Sp: 84.3%) and 1.4 (S: 96.3%; Sp: 84.3%), respectively. These factors were superior to prognostic scores, such as Ranson (AUROC: 0.777; p < 0.001; cut-off: 3.0), BISAP (AUROC: 0.732; p < 0.001; cut-off: 2.0) and Modified Marshall (AUROC: 0.756; p < 0.001; cut-off: 1.0). The mortality rate was 8.8% (16/182), all cases associated with severe AP (17.6%; 16/91). RDW0h and RDW0h-to-serum calcium ratio were higher in nonsurvivor AP patients (15.3 ± 1.4 vs 13.5 ± 1.3; p < 0.001 and 2.0 ± 0.3 vs 1.6 ± 0.3; p < 0.001, respectively). In multivariate and ROC curve analysis, RDW0h (AUROC: 0.842; p < 0.001; cut-off: 14.0), RDW24h (AUROC: 0.848; p < 0.001; cut-off: 13.8) and RDW0h-to-serum calcium ratio (AUROC: 0.820; p < 0.001; cut-off: 1.7) were independent predictors for AP mortality, superior to conventional prognostic scoring systems Ranson (AUROC: 0.640; p = 0.003; cut-off:3.0), BISAP (AUROC: 0.693; p = 0.017; cut-off: 2.0) and Modified Marshall (AUROC: 0.806; p < 0.001; cut-off:1.0).
Conclusions: RDW is a simple routine parameter, available at admission. This AP cohort showed that RDW0h > 13.0 and RDW0h-to-total serum calcium ratio > 1.4 were excellent predictors for severity and RDW0h > 14.0 and RDW0h-to-total serum calcium ratio > 1.7 were very-good predictors for mortality, being superior to conventional prognostic scoring systems.
Keywords: Acute pancreatitis; Mortality; Red cell distribution width; Severity; Total serum calcium.
Conflict of interest statement
Ethics approval and consent to participate
The authors declare that no experiments were performed on humans or animals for this study. The study was approved by the Ethics Committee of Centro Hospitalar e Universitário de Coimbra and was performed in accordance with the Declaration of Helsinki. They have followed the protocols of their work center on the publication of patient data. Patient consent was not obtained since all data was retrieved retrospectively from medical records without additional blood samples or biochemical analysis.
Consent for publication
Not applicable. The authors declare that no patient data (details, images or videos relating to individual participants) are included in this article.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
