

Epidemiology and clinical characteristics of acute respiratory tract infections among hospitalized infants and young children in Chengdu, West China, 2009-2014
- PMID: 29976175
- PMCID: PMC6034247
- DOI: 10.1186/s12887-018-1203-y
Epidemiology and clinical characteristics of acute respiratory tract infections among hospitalized infants and young children in Chengdu, West China, 2009-2014
Abstract
Background: Acute respiratory infection (ARI) is the leading cause of morbidity and mortality in pediatric patients worldwide and imposes an intense pressure on health care facilities. Data on the epidemiology profiles of ARIs are scarce in the western and rural areas of China. The purpose of the current study is to provide data on the presence of potential pathogens of ARIs in hospitalized children in Chengdu, west China.
Methods: Respiratory specimens were obtained from hospitalized patients (under 6 years old) with ARIs in a local hospital in Chengdu. Eight respiratory viruses were identified by PCR and 6 respiratory bacteria by biochemical reactions and Analytical Profile Index (API). Pathogens profiles, clinical characteristics and seasonality were analyzed.
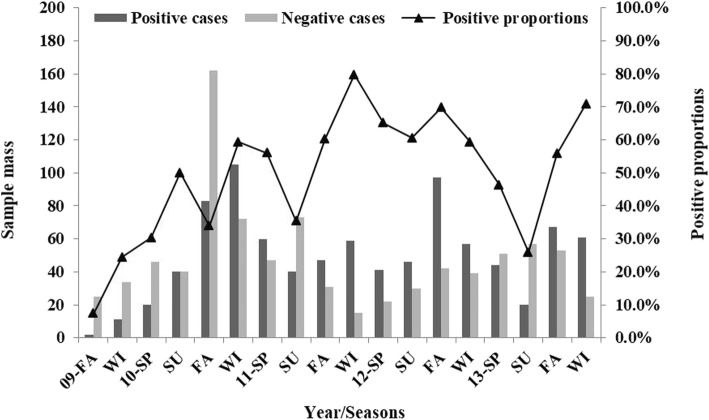
Results: Fifty-one percent of patients were identified with at least one respiratory pathogen. Human rhinovirus (HRV) (23%), Respiratory syncytial virus (RSV) (22.7%) was the most commonly identified viruses, with Klebsiella pneumoniae (11.5%) the most commonly identified bacterium in the study. The presences of more than one pathogen were found, and multiple viral, bacterial, viral/bacterial combinations were identified in 14.9, 3.3 and 13.9% of patients respectively. Respiratory viruses were identified throughout the year with a seasonal peak in December-February. Pathogens profiles and clinical associations were different between infants (< 1 year of age) and older children (> 1 year of age). Infants with ARIs were more likely to have one or more viruses than older children. Infants identified with multiple pathogens had significantly higher proportions of tachypnea than infants that were not.
Conclusions: This study demonstrated that viral agents were frequently found in hospitalized children with ARI in Chengdu during the study period. This study gives us better information on the pathogen profiles, clinical associations, co-infection combinations and seasonal features of ARIs in hospitalized children, which is important for diagnoses and treatment of ARIs, as well as implementation of vaccines in this area. Moreover, future efforts in reducing the impact of ARIs will depend on programs in which available vaccines, especially vaccines on RSV, HRV and S. pneumoniae could be employed in this region and new vaccines could be developed against common pathogens.
Keywords: Acute respiratory infections; Clinical characteristics; Epidemiology; Pediatrics; West China.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Sichuan University, China. Written informed consent was obtained from parents or legal guardians of all participating children.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
