

The prevalence, burden and risk factors associated with bronchial asthma in commonwealth of independent states countries (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study
- PMID: 29976177
- PMCID: PMC6034253
- DOI: 10.1186/s12890-018-0676-7
The prevalence, burden and risk factors associated with bronchial asthma in commonwealth of independent states countries (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study
Abstract
Background: In the Commonwealth of Independent States (CIS) countries epidemiology of Bronchial Asthma (BA) is poorly characterized. The objective of this analysis is to present the prevalence, burden and risk factors associated with BA in the CIS countries as part of the CORE study (Chronic Obstructive REspiratory diseases).
Methods: A total of 2842 adults (≥18 years) were recruited (964 in Kiev, Ukraine, 945 in Almaty, Kazakhstan, and 933 in Baku, Azerbaijan) in 2013-2015 during household visits. A two-step cluster random sampling strategy was used. All respondents were interviewed about respiratory symptoms, smoking, medical history. Two definitions were used: (i) "doctor diagnosed asthma" when the respondent reported that he/she had ever been diagnosed with BA by a doctor, (ii) "wheezing symptoms" (when the respondent reported wheezing at the ATS Respiratory Symptoms Questionnaire during the study) using GINA (2012) recommendations. Chi-square tests were used to assess differences in proportions. Binary logistic regression was used to estimate odds ratios (OR) and 95% CI for association between risk factors and BA.
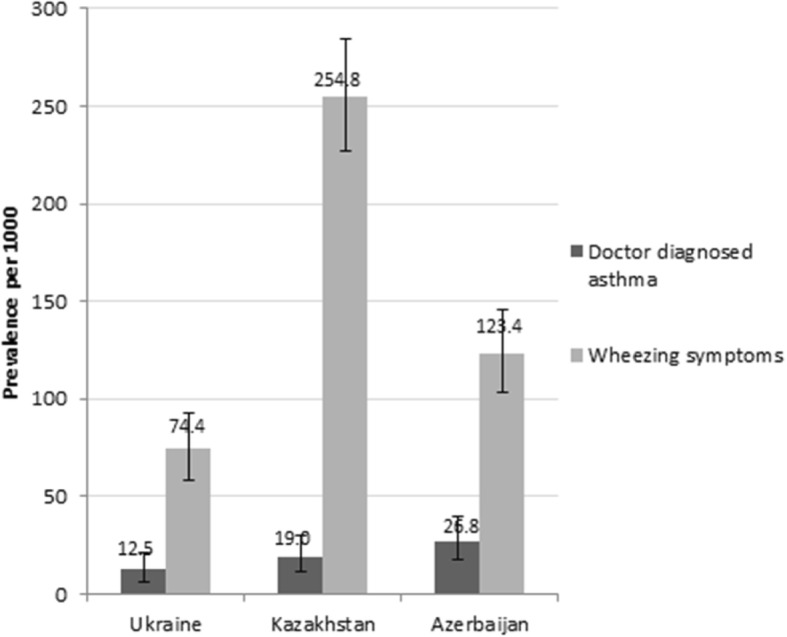
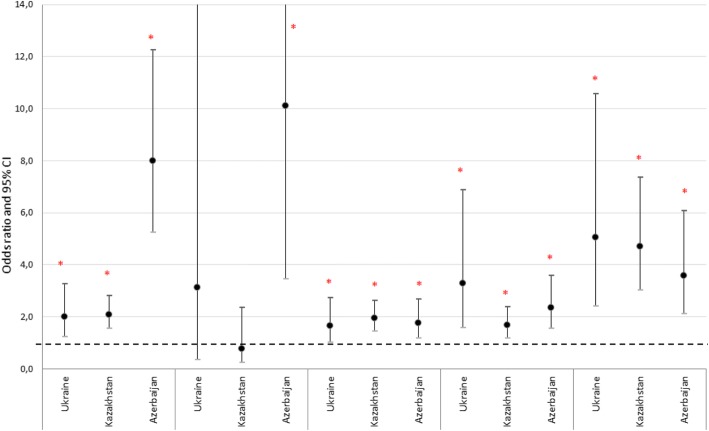
Results: Prevalence of "doctor diagnosed asthma" was 12.5, 19.0 and 26.8 per 1000 persons, and prevalence of "wheezing symptoms" was 74.4, 254.8 and 123.4 per 1000 in Ukraine, Kazakhstan, and Azerbaijan, respectively. Statistically significant relationship with "wheezing symptoms" was shown for smoking (OR 1.99 (CI 1.22-3.27) in Ukraine, 2.08 (CI 1.54-2.81) in Kazakhstan, 8.01 (CI 5.24-12.24) in Azerbaijan); overweight/obesity (OR: 1.66 (CI 1.02-2.72); 1.94 (CI 1.44-2.62); 1.77 (CI 1.18-2.68), respectively) and dusty work (OR: 3.29 (CI 1.57-6.89); 1.68 (CI 1.18-2.39); 2.36 (CI 1.56-3.59), respectively), and for tuberculosis in Azerbaijan (OR: 10.11 (CI 3.44-29.69)). Co-morbidities like hypertension, cardiovascular diseases, abnormal blood lipids and a history of pneumonia occurred significantly (p < 0.05) more frequently in respondents with BA compared to those without BA across all participating countries.
Conclusion: In CIS countries (Ukraine, Kazakhstan and Azerbaijan) the prevalence of doctor diagnosed asthma was significantly lower compared to prevalence of wheezing symptoms underlining that BA is likely to be underreported in these countries. The information provided in this paper will be helpful for healthcare policy makers in CIS countries to instruct BA management strategies and to allocate healthcare resources accordingly.
Keywords: Azerbaijan; Bronchial asthma; Kazakhstan; Prevalence; Risk factors; Ukraine.
Conflict of interest statement
Ethics approval and consent to participate
The study was reviewed and approved by Independent Ethic Committee in Kazakhstan (Central Commission for Ethics at the Ministry of Health of the Republic of Kazakhstan) and by Local Ethic Committees in Kazakhstan, Azerbaijan and Ukraine (Ethic Committee at Semey State Medical University, Almaty, Kazakhstan; Ethic Committee at Scientific Research Institute of Lung Diseases in Baku, Azerbaijan; Commission for Ethics at National Institute of Phthisiology and Pulmonology F.G. Yanovsky of NAMS, Kiev, Ukraine; Commission for Ethics at Center for Primary Health Care #2 of Shevchenko District, Kiev, Ukraine), according to the local legal requirements. Written informed consent was obtained from each participant before any procedures or data collection related to the study.
Consent for publication
Not applicable.
Competing interests
The study was sponsored by GlaxoSmithKline (GSK) marketing a number of treatments for COPD, Allergic Rhinitis, and Asthma.
D. Nugmanova, L. Sokolova, Y. Feshchenko, L. Iashyna, O. Gyrina, I. Mustafayev and G. Aliyeva report grants from GlaxoSmithKline, during the conduct of the study; personal fees from GSK, outside the submitted work; .
J. Makarova, K. Malynovska are employees of GlaxoSmithKline. A. Vasylyev and L. Tariq are GSK employees and shareholder.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- The Global Asthma Report 2014. Auckland, New Zealand: Global Asthma Network, 2014. Available at http://www.globalasthmareport.org
-
- Global Initiative for Asthma (GINA) Global strategy for asthma management and prevention 2012 (update) 2012.
-
- GBD 2015 Chronic Respiratory Disease Collaborators Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived withdisability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Respir Med. 2017;5(9):691–706. doi: 10.1016/S2213-2600(17)30293-X. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
