

The role of deep hypothermic circulatory arrest in surgery for renal or adrenal tumor with vena cava thrombus: a single-institution experience
- PMID: 29976214
- PMCID: PMC6034231
- DOI: 10.1186/s13019-018-0772-z
The role of deep hypothermic circulatory arrest in surgery for renal or adrenal tumor with vena cava thrombus: a single-institution experience
Abstract
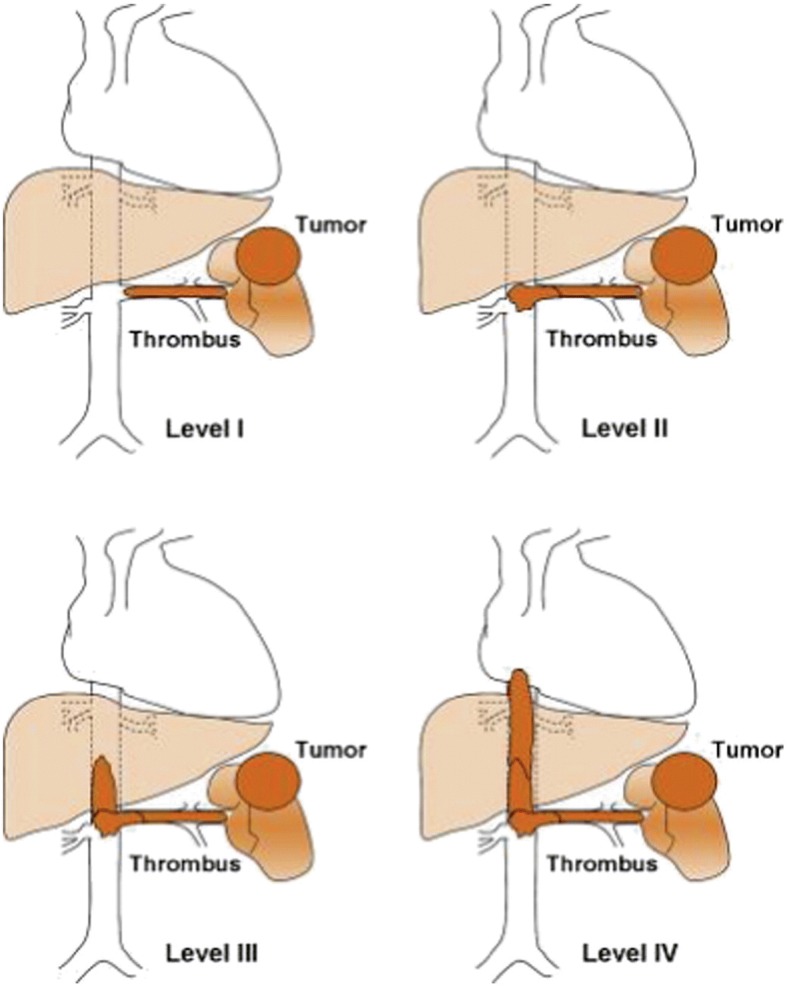
Background: The aim of this study was to review our experience in managing renal or adrenal tumors with level III or IV inferior vena cava thrombus by using deep hypothermic circulatory arrest (DHCA), and to evaluate survival outcomes.
Methods: Between September 2004 and March 2016, we treated 33 patients with renal or adrenal malignancy tumor and thrombus extending into the inferior vena cava. Patients were identified according to radiographic records and operative findings. Clinicopathological and operative characteristics were recorded, and comparisons of clinical and operative characteristics through DHCA were performed. A Cox regression model was used to determine predictors of perioperative mortality.
Results: Twenty-one out of 33 patients with level III (n = 15), level IV (n = 5), or level II (n = 1) renal or adrenal tumors were treated surgically through cardiopulmonary bypass (CPB) with DHCA, and 12 patients with level II or III tumors were treated surgically through normothermic CPB. Three complications were observed, and one death occurred perioperatively, owing to multiple organ failure. The overall perioperative mortality was 4.7%. There were significant differences in the clinicopathological characteristics, operative duration, estimated blood loss, transfusions and hospital stay depending on use of DHCA. Multivariate analysis indicated that the operative duration (OR, 3.78; P < 0.001), estimated blood loss (OR, 1.08; P = 0.02), and transfusion (OR, 2.13; P = 0.038) during/after surgery were positively associated with higher mortality and morbidity. DHCA failed to reach statistical significance (P = 0.378).
Conclusions: Use of CPB and DHCA to treat renal or adrenal tumors allows for complete tumor resection, especially at the T4 stage. Although it can cause physical damage, this technique does not increase operative risk and is a relatively safe approach.
Keywords: Cardiopulmonary bypass; Hypothermic arrest; Renal tumor; Thrombectomy.
Conflict of interest statement
Ethics approval and consent to participate
Study protocol was approved by the Ethical Committee of the NanFang Hospital, Southern Medical University.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Chiappini B, Savini C, Marinelli G, Suarez SM, Di Eusanio M, Fiorani V, Pierangeli A. Cavoatrial tumor thrombus: single-stage surgical approach with profound hypothermia and circulatory arrest, including a review of the literature. J Thorac Cardiovasc Surg. 2002;124:684–688. doi: 10.1067/mtc.2002.124295. - DOI - PubMed
-
- Lawindy SM, Kurian T, Kim T, Mangar D, Armstrong PA, Alsina AE, Sheffield C, Sexton WJ, Spiess PE. Important surgical considerations in the management of renal cell carcinoma (RCC) with inferior vena cava (IVC) tumour thrombus. BJU Int. 2012;110:926–939. doi: 10.1111/j.1464-410X.2012.11174.x. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
