

Achieving optimal technology and behavioral uptake of single and combined interventions of water, sanitation hygiene and nutrition, in an efficacy trial (WASH benefits) in rural Bangladesh
- PMID: 29976251
- PMCID: PMC6034207
- DOI: 10.1186/s13063-018-2710-8
Achieving optimal technology and behavioral uptake of single and combined interventions of water, sanitation hygiene and nutrition, in an efficacy trial (WASH benefits) in rural Bangladesh
Abstract
Background: Uptake matters for evaluating the health impact of water, sanitation and hygiene (WASH) interventions. Many large-scale WASH interventions have been plagued by low uptake. For the WASH Benefits Bangladesh efficacy trial, high uptake was a prerequisite. We assessed the degree of technology and behavioral uptake among participants in the trial, as part of a three-paper series on WASH Benefits Intervention Delivery and Performance.
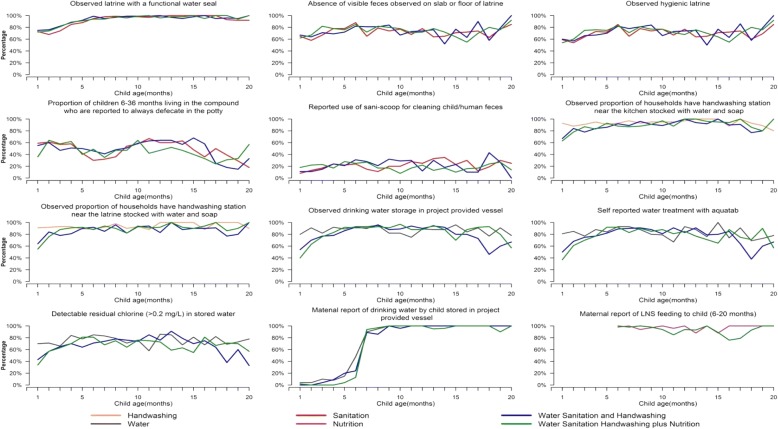
Methods: This study is a cluster randomized trial comprised of geographically matched clusters among four districts in rural Bangladesh. We randomly allocated 720 clusters of 5551 pregnant women to individual or combined water, sanitation, handwashing, and nutrition interventions, or a control group. Behavioral objectives included; drinking chlorine-treated, safely stored water; use of a hygienic latrine and safe feces disposal at the compound level; handwashing with soap at key times; and age-appropriate nutrition behaviors (pregnancy to 24 months) including a lipid-based nutrition supplement (LNS). Enabling technologies and behavior change were promoted by trained local community health workers through periodic household visits. To monitor technology and behavioral uptake, we conducted surveys and spot checks in 30-35 households per intervention arm per month, over a 20-month period, and structured observations in 324 intervention and 108 control households, approximately 15 months after interventions commenced.
Results: In the sanitation arms, observed adult use of a hygienic latrine was high (94-97% of events) while child sanitation practices were moderate (37-54%). In the handwashing arms, handwashing with soap was more common after toilet use (67-74%) than nonintervention arms (18-40%), and after cleaning a child's anus (61-72%), but was still low before food handling. In the water intervention arms, more than 65% of mothers and index children were observed drinking chlorine-treated water from a safe container. Reported LNS feeding was > 80% in nutrition arms. There was little difference in uptake between single and combined intervention arms.
Conclusions: Rigorous implementation of interventions deployed at large scale in the context of an efficacy trial achieved high levels of technology and behavioral uptake in individual and combined WASH and nutrition intervention households. Further work should assess how to achieve similar uptake levels under programmatic conditions.
Trial registration: WASH Benefits Bangladesh: ClinicalTrials.gov, identifier: NCT01590095 . Registered on April 30, 2012.
Keywords: Bangladesh; Behavior change; Child nutrition; Cluster randomized controlled trial; Efficacy; Handwashing; Intervention uptake; Sanitation; WASH benefits; Water quality.
Conflict of interest statement
Ethics approval and consent to participate
All households provided written informed consent at enrollment. The protocol was reviewed and approved by human subjects review committees at the icddr,b and at the University of California, Berkeley.
Consent for publication
All co-authors have reviewed this version of the manuscript and provided consent for manuscript submission.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
