

Beet the Best?
- PMID: 29976553
- PMCID: PMC6202165
- DOI: 10.1161/CIRCRESAHA.118.313131
Beet the Best?
Abstract
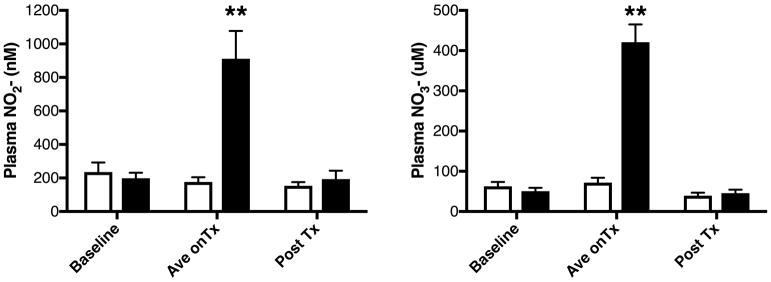
Rationale: A primary goal of therapy for patients with peripheral artery disease (PAD) and intermittent claudication is increased ambulatory function. Supervised exercise rehabilitation was recently shown to confer superior walking benefits to pharmacological or surgical interventions. Increases in plasma inorganic nitrite, via oral nitrate, have been shown to increase exercise performance in both human and animal models, especially in hypoxic conditions.
Objective: To determine whether a 36-session exercise rehabilitation program while consuming oral inorganic nitrate (4.2 mmol concentrated beetroot juice) would produce superior benefits over exercise plus placebo in pain-free walking and markers of increased skeletal muscle perfusion in patients with PAD and intermittent claudication.
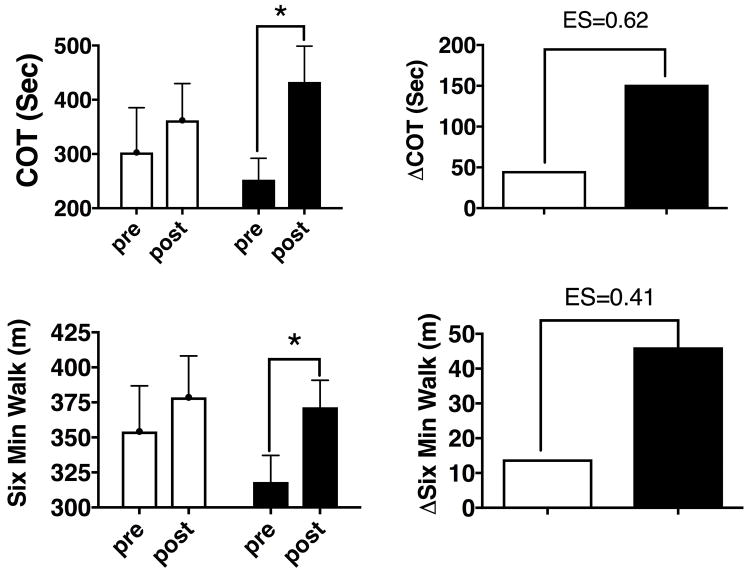
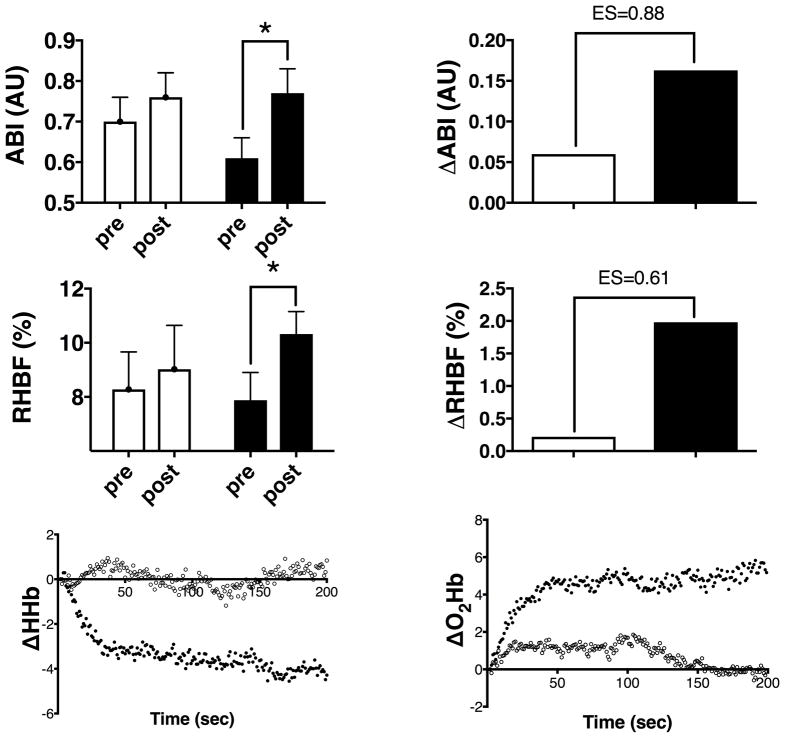
Methods and results: This was a randomized, double-blind, per-protocol study design. After the 12-week protocol, claudication onset time on a maximal treadmill test increased by 59.2±57.3 s for the exercise plus placebo group (n=13) and by 180.3±46.6 s for the exercise plus beetroot juice group (n=11; P≤0.05). This produced a between treatment medium to large standardized effect size (Cohen d) of 0.62 (95% CI, -0.23 to +1.44). The data for 6-minute walk distance showed a similar pattern with increases of 24.6±12.1 and 53.3±19.6 m ( P≤0.05) in the exercise plus placebo and exercise plus beetroot juice groups, respectively. Measures of gastrocnemius perfusion, including ankle-brachial index, peak reactive hyperemic blood flow, and tissue deoxygenation characteristics, during exercise (assessed my near-infrared spectroscopy) all changed significantly for the exercise plus beetroot juice group with moderate-to-large effect sizes over exercise plus placebo changes.
Conclusions: Although it is premature to speculate on overall clinical utility of a nitrate-based therapy for PAD, this early pilot study evidence is encouraging. Specifically, our data suggests that increasing plasma nitrite before exercise may allow PAD subjects to train with less pain, at higher workloads for longer durations at each training session, thereby maximizing the beneficial peripheral vascular and skeletal muscle adaptations.
Clinical trial registration: URL: http://www.clinicaltrials.gov . Unique identifier: NCT01684930 and NCT01785524.
Keywords: exercise; humans; inorganic nitrate; nitric oxide; peripheral artery disease.
Figures
Comment in
-
"Beet It".Circ Res. 2018 Aug 31;123(6):635-637. doi: 10.1161/CIRCRESAHA.118.313667. Circ Res. 2018. PMID: 30355240 Free PMC article. No abstract available.
References
-
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UKA, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. The Lancet. 2013;382:1329–1340. - PubMed
-
- Mahoney EM, Wang K, Keo HH, Duval S, Smolderen KG, Cohen DJ, Steg G, Bhatt DL, Hirsch AT. Vascular Hospitalization Rates and Costs in Patients With Peripheral Artery Disease in the United States. Circulation: Cardiovascular Quality and Outcomes. 2010;3:642–651. - PubMed
-
- Sieminski DJ, Gardner AW. The Relationship between Free-Living Daily Physical Activity and the Severity of Peripheral Arterial Occlusive Disease. Vascular Medicine. 1997;2:286–291. - PubMed
-
- Olsen P, Gustafsen J, Rasmussen L, Lorentzen J. Long-term results after arterial surgery for arteriosclerosis of the lower limbs in young adults. Eur J Vasc Surg. 1988;2:15–18. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
