

CD16+NK-92 and anti-CD123 monoclonal antibody prolongs survival in primary human acute myeloid leukemia xenografted mice
- PMID: 29976748
- PMCID: PMC6165813
- DOI: 10.3324/haematol.2017.187385
CD16+NK-92 and anti-CD123 monoclonal antibody prolongs survival in primary human acute myeloid leukemia xenografted mice
Abstract
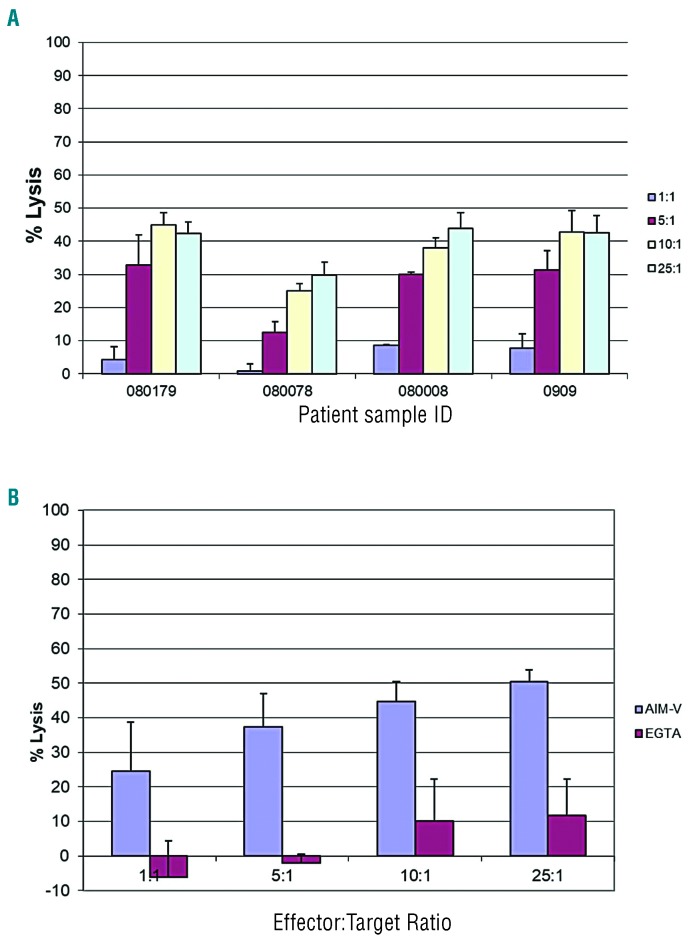
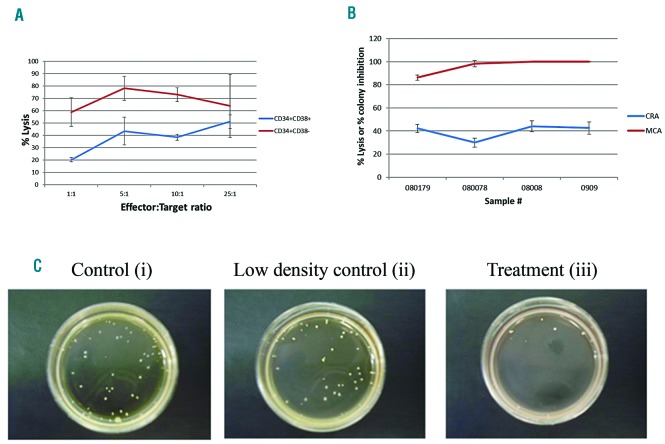
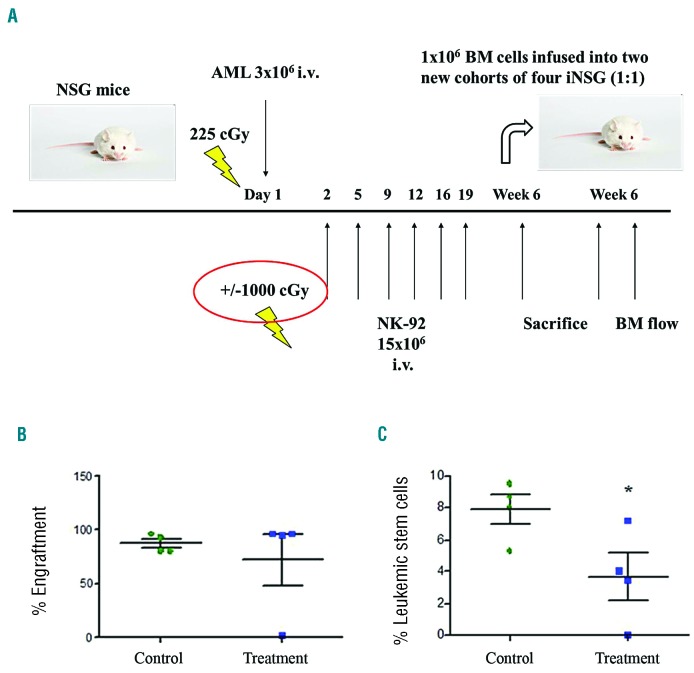
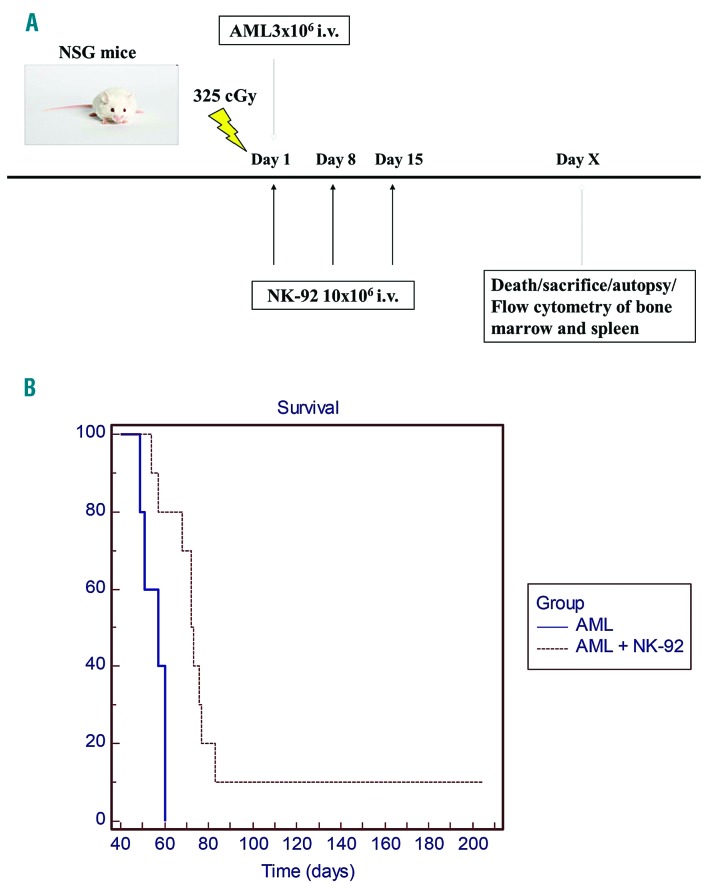
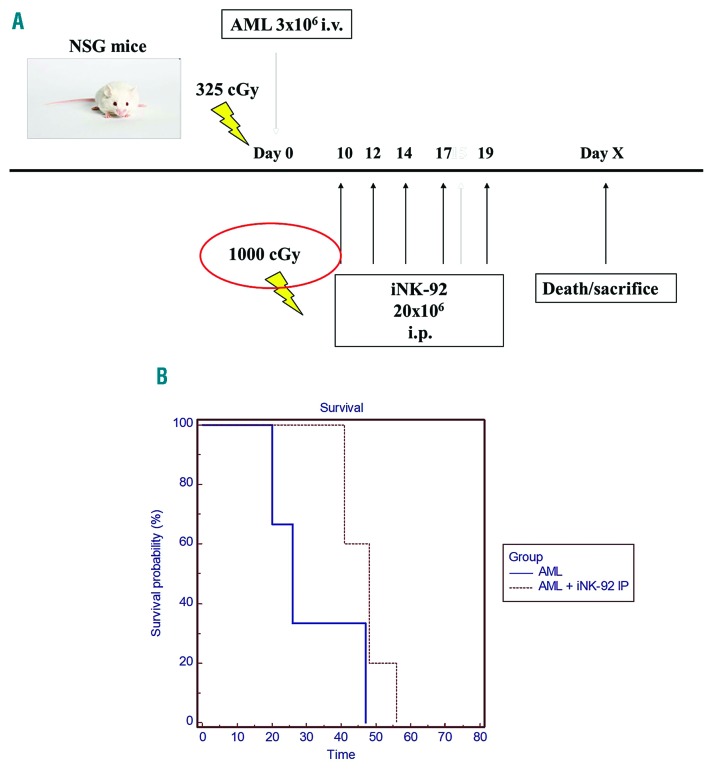
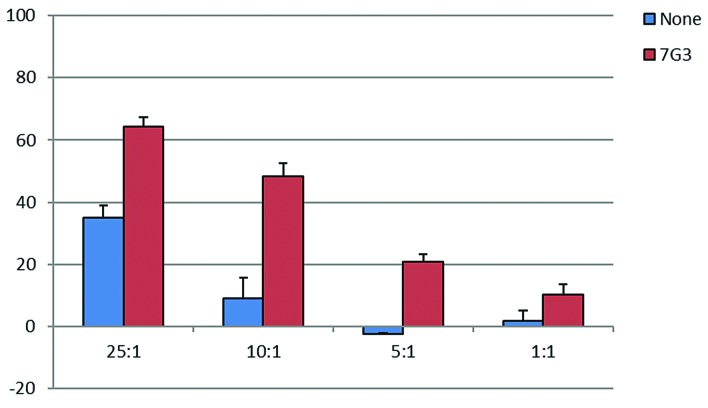
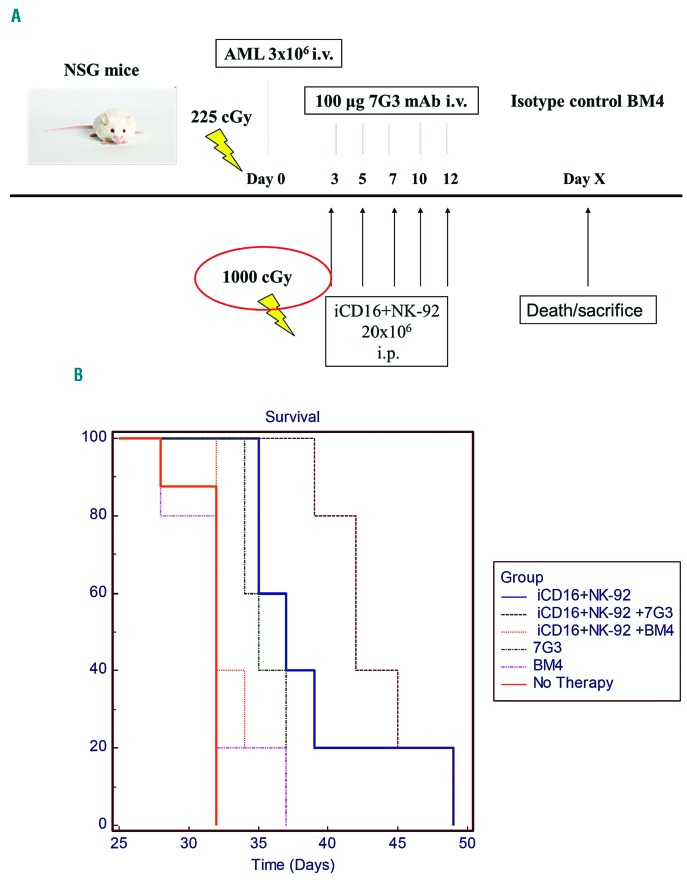
Patients with acute myeloid leukemia (AML) often relapse after initial therapy because of persistence of leukemic stem cells that frequently express the IL-3 receptor alpha chain CD123. Natural killer (NK) cell-based therapeutic strategies for AML show promise and we explore the NK cell lines, NK-92 and CD16+ NK-92, as a treatment for AML. NK-92 has been tested in phase I clinical trials with minimal toxicity; irradiation prior to infusion prevents risk of engraftment. The CD16 negative NK-92 parental line was genetically modified to express the high affinity Fc gamma receptor, enabling antibody-dependent cell-mediated cytotoxicity, which we utilized in combination with an anti-CD123 antibody to target leukemic stem cells. NK-92 was preferentially cytotoxic against leukemic stem and progenitor cells compared with bulk leukemia in in vitro assays, while CD16+ NK-92 in combination with an anti-CD123 mAb mediated antibody-dependent cell-mediated cytotoxicity against CD123+ leukemic targets. Furthermore, NK-92 infusions (with or without prior irradiation) improved survival in a primary AML xenograft model. Mice xenografted with primary human AML cells had a superior survival when treated with irradiated CD16+NK-92 cells and an anti-CD123 monoclonal antibody (7G3) versus treatment with irradiated CD16+NK-92 cells combined with an isotype control antibody. In this proof-of-principle study, we show for the first time that a CD16+NK-92 cell line combined with an antibody that targets a leukemic stem cell antigen can lead to improved survival in a relevant pre-clinical model of AML.
Copyright © 2018 Ferrata Storti Foundation.
Figures
References
-
- Hurwitz CA, Mounce KG, Grier HE. Treatment of patients with acute myelogenous leukemia: review of clinical trials of the past decade. J Pediatr Hematol Oncol. 1995;17(3):185–197. - PubMed
-
- Lowenberg B, Downing JR, Burnett A. Acute myeloid leukemia. N Engl J Med. 1999;341(14):1051–1062. - PubMed
-
- Ribeiro RC, Razzouk BI, Pounds S, Hijiya N, Pui CH, Rubnitz JE. Successive clinical trials for childhood acute myeloid leukemia at St Jude Children’s Research Hospital, from 1980 to 2000. Leukemia. 2005; 19(12):2125–2129. - PubMed
-
- Lapidot T, Sirard C, Vormoor J, et al. A cell initiating human acute myeloid leukaemia after transplantation into SCID mice. Nature. 1994;367(6464):645–648. - PubMed
-
- Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3(7):730–737. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
