

Innate and adaptive immune dysregulation in critically ill ICU patients
- PMID: 29976949
- PMCID: PMC6033948
- DOI: 10.1038/s41598-018-28409-7
Innate and adaptive immune dysregulation in critically ill ICU patients
Abstract
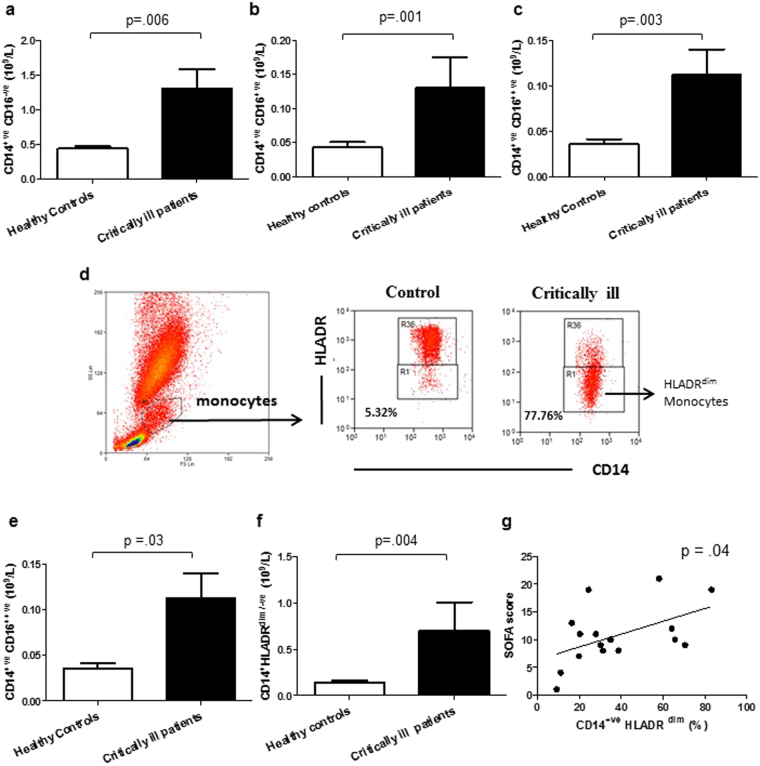
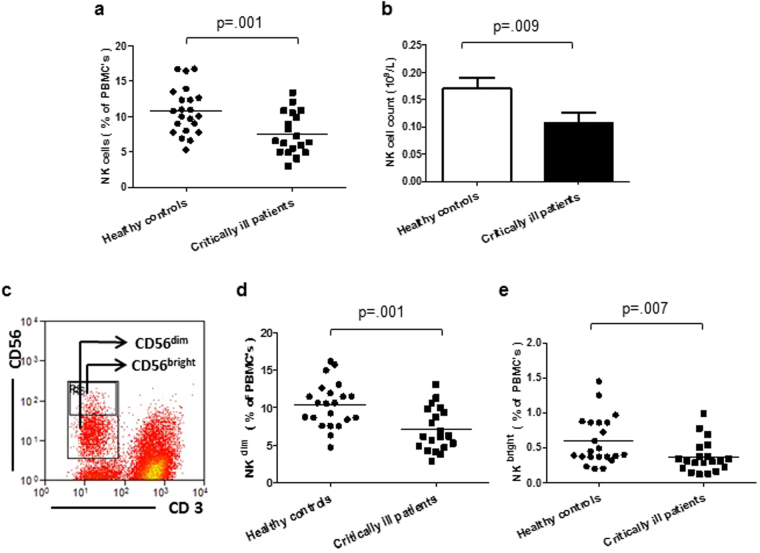
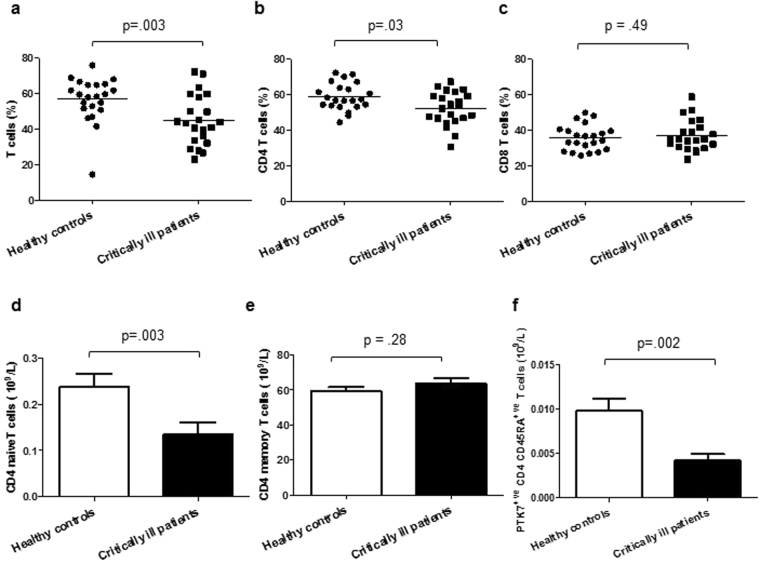
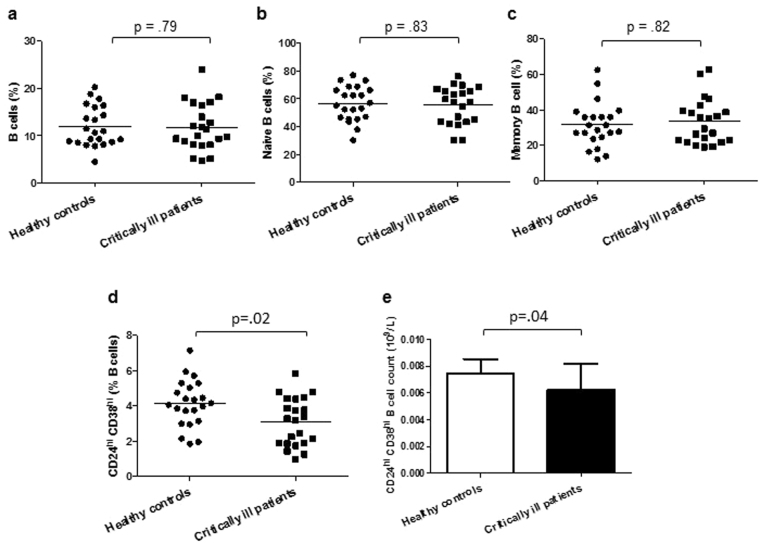
This study aimed to evaluate whether ICU patients who developed persistent critical illness displayed an immune profile similar to an aged immune phenotype and any associations with patient outcomes. Twenty two critically ill ICU patients (27-76 years, 15 males), at day 5 of mechanical ventilation, and 22 healthy age-matched controls (27-77 years, 13 males) were recruited. Frequency and phenotype of innate and adaptive immune cells and telomere length in peripheral blood mononuclear cells (PBMCs) were measured. An elevated granulocyte count (p < 0.0001), increased numbers of immature granulocytes (p < 0.0001), increased CD16++ve monocytes (p = 0.003) and CD14+ve HLADRdim/low monocytes (p = 0.004) and lower NK cell numbers (p = 0.007) were observed in ICU patients compared to controls. Critically ill patients also had lower numbers of total T lymphocytes (p = 0.03), naïve CD4 T cells (p = 0.003) and PTK7+ve recent thymic emigrants (p = 0.002), and increased senescent CD28-ve CD57+ve CD4 T cells (p = 0.02), but there was no difference in PBMC telomere length. Regulatory immune cell frequency was affected with reduced circulating CD19+veCD24hiCD38hi regulatory B cells (p = 0.02). However, only a raised neutrophil:lymphocyte ratio and reduced frequency of CD14+ve HLADRdim/low monocytes were associated with poor outcomes. We conclude that persistent critical illness results in changes to immune cell phenotype only some of which are similar to that seen in physiological ageing of the immune system.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Hospital Episode Statistics Analysis H. Adult Critical Care in England - April 2013 to March 2014. Health and Social Care Information Centre. (2015).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
