

A novel endoscopic classification for craniopharyngioma based on its origin
- PMID: 29977006
- PMCID: PMC6033946
- DOI: 10.1038/s41598-018-28282-4
A novel endoscopic classification for craniopharyngioma based on its origin
Abstract
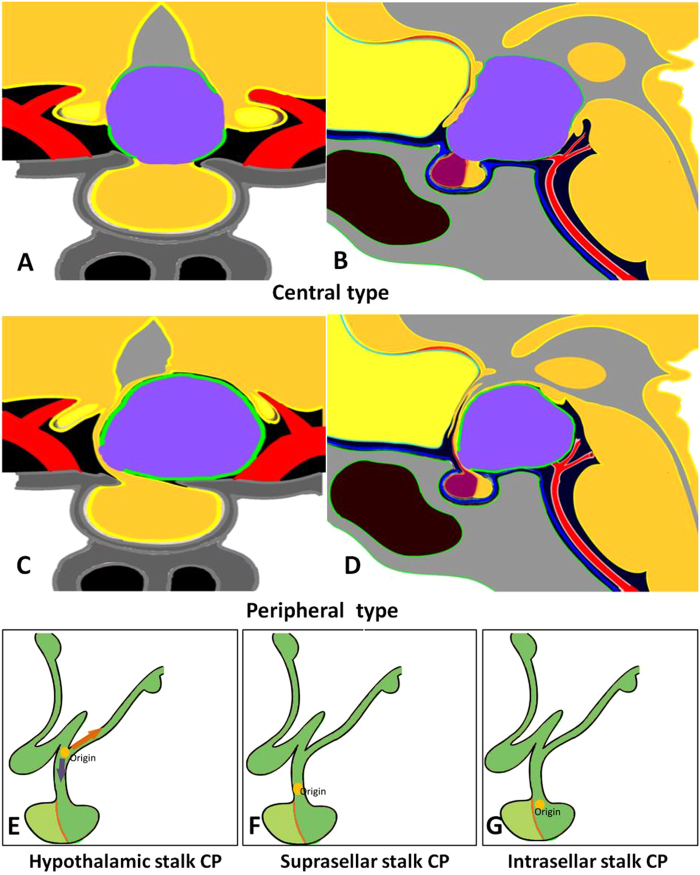
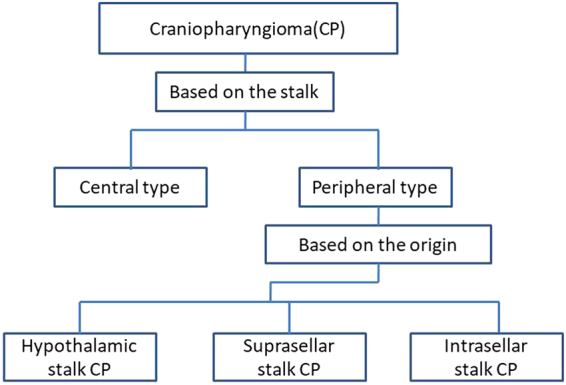
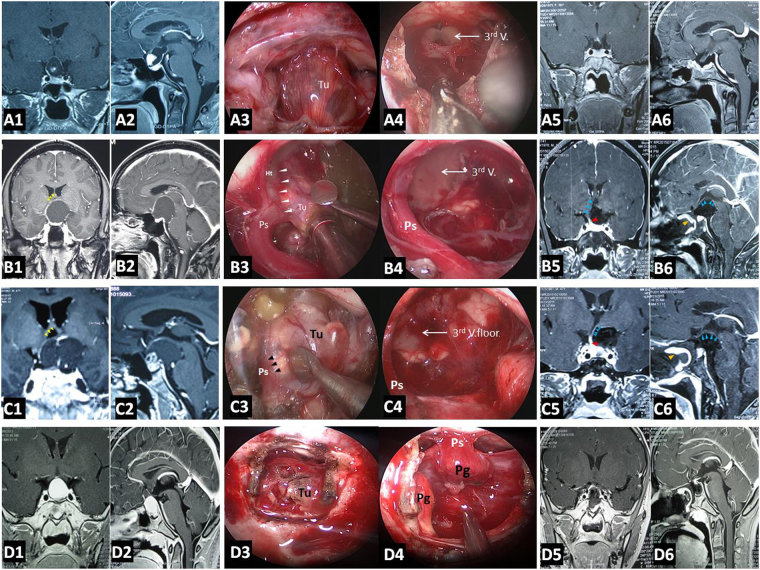
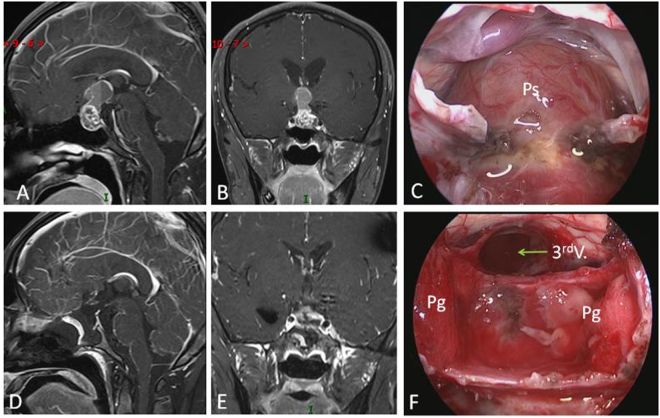
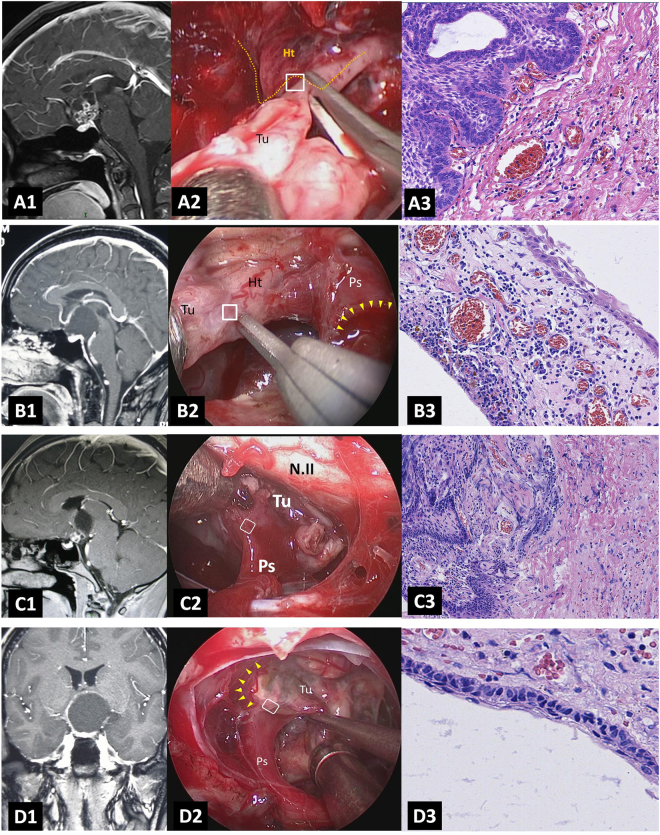
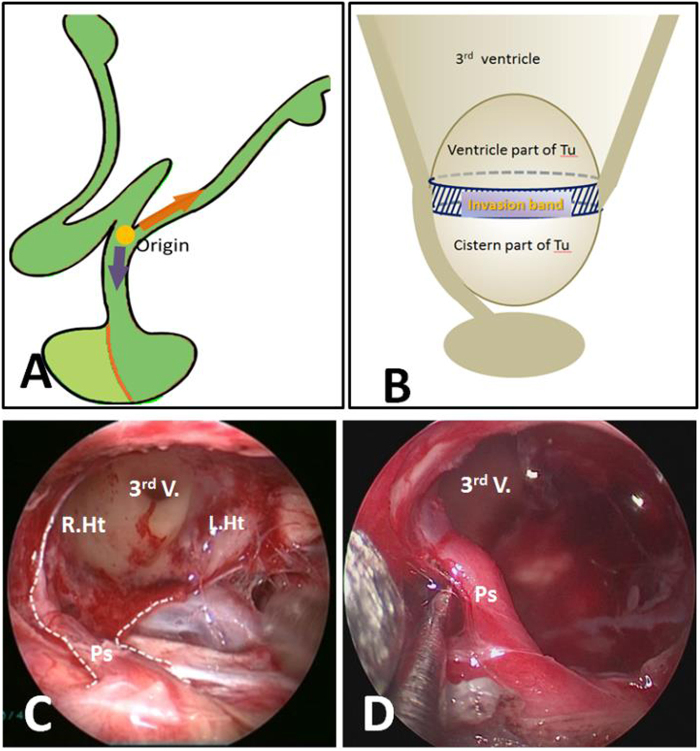
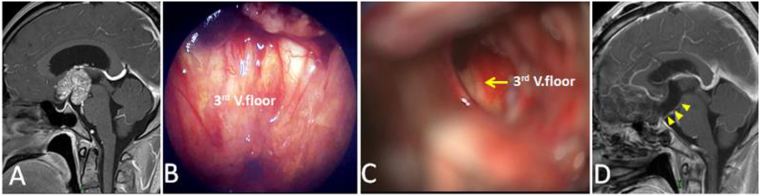
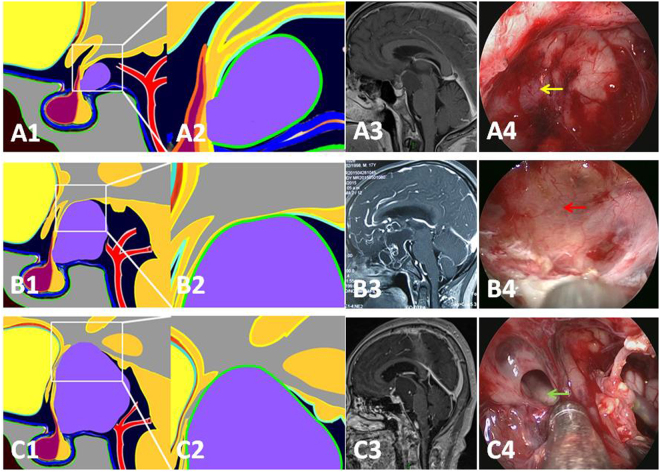
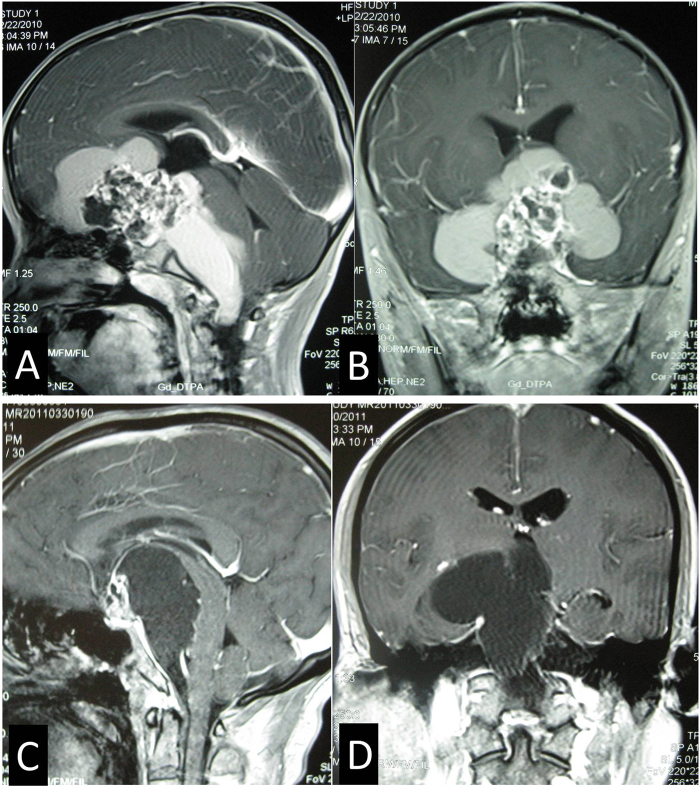
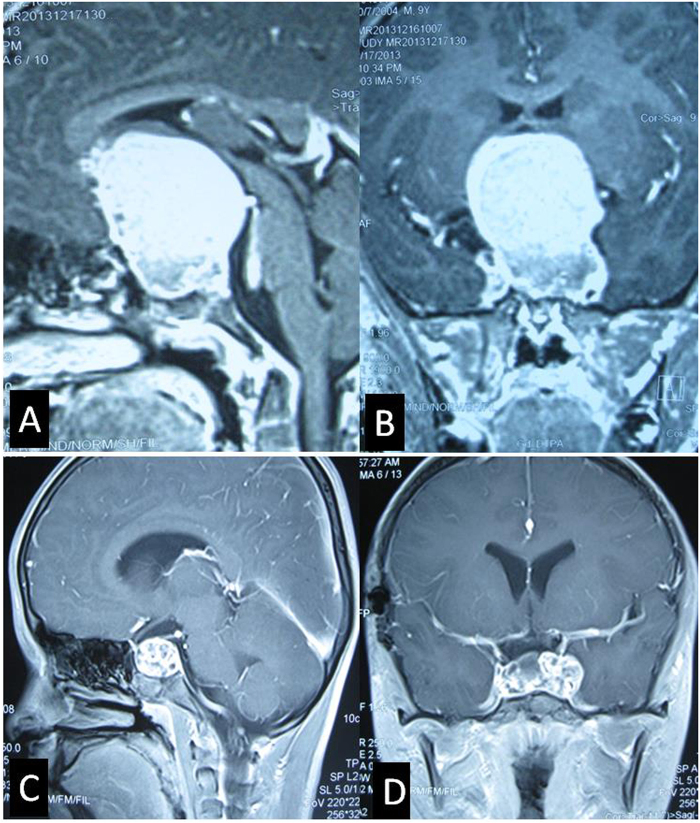
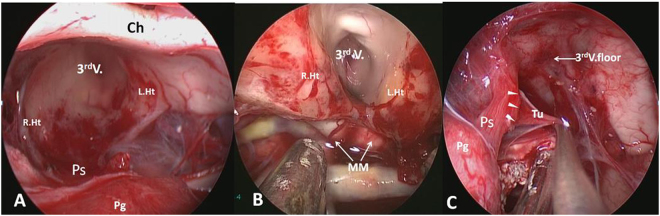
Endoscopic endonasal approach for craniopharyngioma (CP) resection provides a wide view and direct observation of hypothalamus and origin of tumor. Under endoscopy, 92 CPs were classified into 2 types: Peripheral and Central, according to its relation to pituitary stalk. Peripheral type was further divided into 3 subtypes: Hypothalamic stalk, Suprasellar stalk and Intrasellar stalk CP, according to the different origin site along hypothalamus-pituitary axis. Peripheral type arisen from the stalk but expanded and grown laterally in an exophytic pattern, accounting for 71.7% of all CPs, preservation rate of stalk was higher (76.0%). Central type grew within and along pituitary stalk and located strictly in the midline. The pituitary stalk was hardly preserved (only15.4%). Hypothalamic stalk CPs (n = 36, 54.6%) developed from the junction of hypothalamus and stalk, hypothalamus damage was found in all of this subtype after surgery. Suprasellar stalk CPs (n = 14, 21.2%) originated from the lower portion of stalk and displaced hypothalamus upward rather than infiltrated it. Intrasellar stalk CPs (n = 16, 24.2%) arose from the subdiaphragma portion of the stalk, with less hypothalamus damage. Recoginzing the origin of CP is helpful to understand its growth pattern and relation to hypothalamus, which is critical in planning the most appropriate surgical approach and degree of excision.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
