

Closed Or Open after Source Control Laparotomy for Severe Complicated Intra-Abdominal Sepsis (the COOL trial): study protocol for a randomized controlled trial
- PMID: 29977328
- PMCID: PMC6015449
- DOI: 10.1186/s13017-018-0183-4
Closed Or Open after Source Control Laparotomy for Severe Complicated Intra-Abdominal Sepsis (the COOL trial): study protocol for a randomized controlled trial
Abstract
Background: Severe complicated intra-abdominal sepsis (SCIAS) has an increasing incidence with mortality rates over 80% in some settings. Mortality typically results from disruption of the gastrointestinal tract, progressive and self-perpetuating bio-mediator generation, systemic inflammation, and multiple organ failure. Principles of treatment include early antibiotic administration and operative source control. A further therapeutic option may be open abdomen (OA) management with active negative peritoneal pressure therapy (ANPPT) to remove inflammatory ascites and ameliorate the systemic damage from SCIAS. Although there is now a biologic rationale for such an intervention as well as non-standardized and erratic clinical utilization, this remains a novel therapy with potential side effects and clinical equipoise.
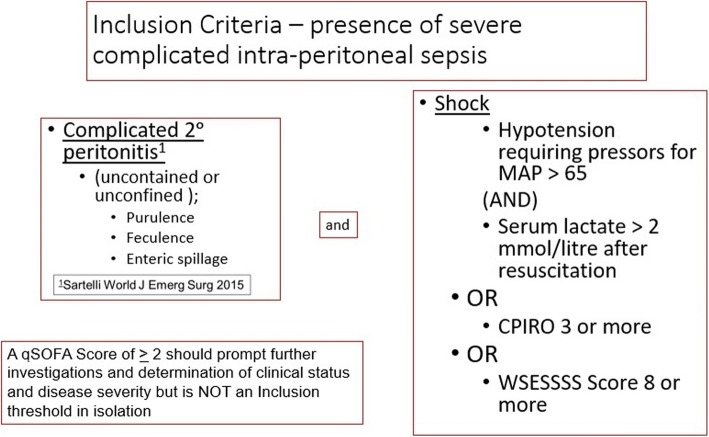
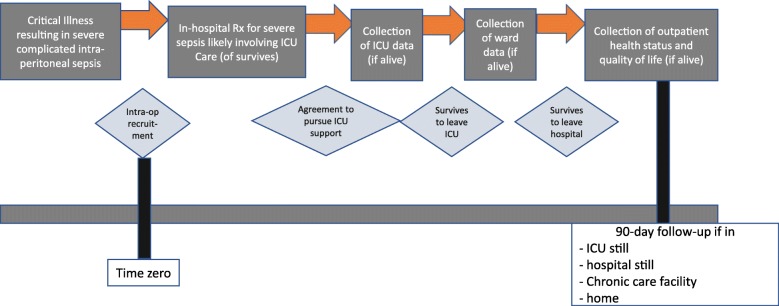
Methods: The Closed Or Open after Laparotomy (COOL) study will constitute a prospective randomized controlled trial that will randomly allocate eligible surgical patients intra-operatively to either formal closure of the fascia or use of the OA with application of an ANPTT dressing. Patients will be eligible if they have free uncontained intra-peritoneal contamination and physiologic derangements exemplified by septic shock OR a Predisposition-Infection-Response-Organ Dysfunction Score ≥ 3 or a World-Society-of-Emergency-Surgery-Sepsis-Severity-Score ≥ 8. The primary outcome will be 90-day survival. Secondary outcomes will be logistical, physiologic, safety, bio-mediators, microbiological, quality of life, and health-care costs. Secondary outcomes will include days free of ICU, ventilation, renal replacement therapy, and hospital at 30 days from the index laparotomy. Physiologic secondary outcomes will include changes in intensive care unit illness severity scores after laparotomy. Bio-mediator outcomes for participating centers will involve measurement of interleukin (IL)-6 and IL-10, procalcitonin, activated protein C (APC), high-mobility group box protein-1, complement factors, and mitochondrial DNA. Economic outcomes will comprise standard costing for utilization of health-care resources.
Discussion: Although facial closure after SCIAS is considered the current standard of care, many reports are suggesting that OA management may improve outcomes in these patients. This trial will be powered to demonstrate a mortality difference in this highly lethal and morbid condition to ensure critically ill patients are receiving the best care possible and not being harmed by inappropriate therapies based on opinion only.
Trial registration: ClinicalTrials.gov, NCT03163095.
Keywords: Bio-mediators; Intra-peritoneal sepsis; Laparotomy; Multiple organ dysfunction; Open-abdomen; Peritonitis; Randomized trial; Septic shock.
Conflict of interest statement
The COOL trial has been ethically approved at the lead and pilot center by the Conjoint Health Research Ethics Board (CHREB) of the University of Calgary (REB16-1588). The study has also been registered with the National Institutes of Health (ClinicalTrials.gov, identifier: NCT03163095).Andrew W. Kirkpatrick serves in the Canadian Forces Medical Services and has consulted for the Innovative Trauma Care and Acelity Corporations. Jessica L. McKee declares that she has consulted for Innovative Trauma Care, Aceso, and the Acelity Corporations. Osvaldo Chiara reported having consulted for the Acelity Corporation. Jose J. Diaz reported having consulted for the Acelity Corporation. Michael Sugrue reported having consulted for the Smith and Nephew Corporation. Ernest E. Moore reported Research support and intellectual property related to the Haemonetics, TEM Systems, Pryor Corporations, and being a Cofounder of Thrombo Therapeutics Inc. The remaining authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcomes, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
