

Sepsis in a Panorama: What the Cardiovascular Physician Should Know
- PMID: 29977465
- PMCID: PMC6027712
- DOI: 10.14797/mdcj-14-2-89
Sepsis in a Panorama: What the Cardiovascular Physician Should Know
Abstract
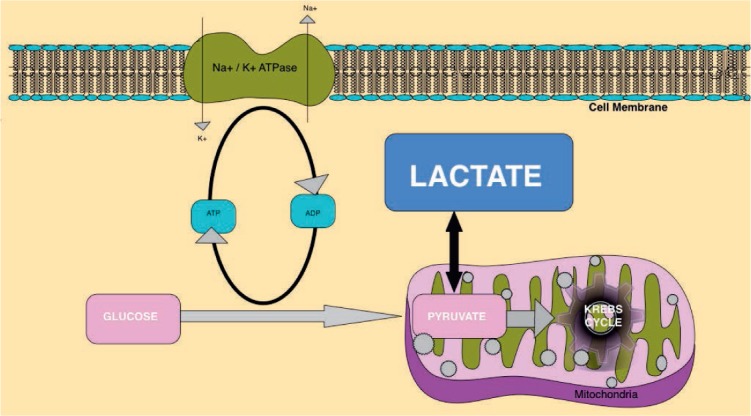
Sepsis accounts for an estimated 30 million cases and 6 million deaths globally each year. According to a multidisciplinary task force convened by the Society of Critical Care Medicine and European Society of Intensive Care Medicine, sepsis is defined as life-threatening organ dysfunction due to a dysregulated host response to infection. Sepsis is a medical emergency, so much so that the World Health Organization made it a global health priority. Since patients with cardiovascular diseases have unique risk factors for sepsis, prompt and accurate diagnosis is critical. In this regard, the sepsis-specific Sequential Organ Failure Assessment (SOFA) helps clinicians identify the organ dysfunction and predict outcomes. Sepsis management is grouped into specific interventions called bundles, and completion of each bundle element is time sensitive. The U.S. Centers for Medicaid and Medicare Services and some state-specific regulations have made compliance with these bundles reportable as a quality measure. The updated Surviving Sepsis Campaign Hour-1 bundle recommends that lactate measurement, blood cultures procurement, broad spectrum antibiotics administration, resuscitation with 30 mL/kg crystalloid, and vasopressor initiation for hypotension all be initiated within 1 hour of time zero, which is from the time of triage in the emergency department or from sepsis diagnosis. Septic shock is defined as hypotension with a mean arterial pressure less than 65 mm Hg, requiring vasopressors despite adequate fluid resuscitation and/or lactic acid levels above 2 mmol/L. Both fluid resuscitation and clinical re-evaluation with lactate measurement guide the fluid and vasopressor therapy. Specific guidelines exist for organ support that address mechanical ventilation, blood transfusions, vasopressor choices, and nutrition.
Keywords: SOFA; lactate; qSOFA; sepsis; sepsis bundles; septic shock; vasopressor.
Conflict of interest statement
Conflict of Interest Disclosure: The author has completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NK, . et al. .; International Forum of Acute Care Trialists Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am J Respir Crit Care Med. 2016. February 1; 193 3: 259– 72. - PubMed
-
- Torio CM, Moore BJ. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013: Statistical Brief #204. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006–2016. May. - PubMed
-
- Rowan KM, Angus DC, Bailey M, . et al. .; PRISM Investigators Early, Goal-Directed Therapy for Septic Shock - A Patient-Level Meta-Analysis. N Engl J Med. 2017. June 8; 376 23: 2223– 34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
