

Is 24/7 In-House Intensivist Staffing Necessary in the Intensive Care Unit?
- PMID: 29977470
- PMCID: PMC6027728
- DOI: 10.14797/mdcj-14-2-134
Is 24/7 In-House Intensivist Staffing Necessary in the Intensive Care Unit?
Abstract
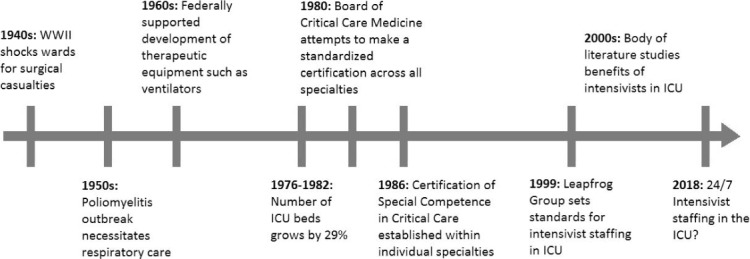
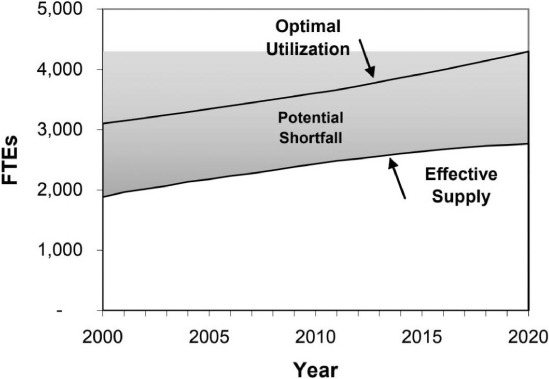
Over the past few decades, an increasing number of studies have shown that intensivist-staffed intensive care units (ICUs) lead to overall economic benefits and improved patient outcomes, including shorter length of stay and lower rates of complications and mortality. This body of evidence has convinced advocacy groups to adopt this staffing model as a standard of care in the ICU so that more hospitals are offering around-the-clock intensivist coverage. Even so, opponents have pointed to high ICU staffing costs and a shortage of physicians trained in critical care as barriers to implementing this model. While these arguments may hold true in low-acuity, low-volume ICUs, evidence has shown that in high-acuity, high-volume centers such as teaching hospitals and tertiary care centers, the benefits outweigh the costs. This article explores the history of intensivists and critical care, the arguments for 24/7 ICU staffing, and outcomes in various ICU settings but is not intended to be a comprehensive review of all controversies surrounding continuous ICU staffing.
Keywords: 24/7 staffing; ICU; advanced practice provider; critical care unit; intensive care unit; intensivist.
Conflict of interest statement
Conflict of Interest Disclosure: Dr. Masud is a consultant for Mallinckrodt Pharmaceuticals and Chiesi USA, Inc.
Figures
References
-
- Kelley MA. Critical care medicine–a new specialty? N Engl J Med. 1988. June 16; 318 24: 1613– 7. - PubMed
-
- Li TC, Phillips MC, Shaw L, Cook EF, Natanson C, Goldman L.. On-site physician staffing in a community hospital intensive care unit. Impact on test and procedure use and on patient outcome. JAMA. 1984. October 19; 252 15: 2023– 7. - PubMed
-
- Carson SS, Stocking C, Podsadecki T, . et al. Effects of organizational change in the medical intensive care unit of a teaching hospital: a comparison of ‘open’ and ‘closed’ formats. JAMA. 1996. July 24–31; 276 4: 322– 8. - PubMed
-
- Multz AS, Chalfin DB, Samson IM, . et al. A “closed” medical intensive care unit (MICU) improves resource utilization when compared with an “open” MICU. Am J Respir Crit Care Med. 1998. May; 157 5 Pt 1: 1468– 73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
